
Abstract
Objective
Prophylactic pancreatic duct (PD) stent placement has been shown to reduce the incidence of post-ERCP pancreatitis (PEP) especially in high-risk patients. However, there is no consensus on the best type of PD stent. The purpose of our study was to evaluate the differences in the outcomes between long (>3 cm) pigtail and short (≤3 cm) flanged 4 Fr Freeman Pancreatic Flexi-Stents in preventing PEP.
Methods
We retrospectively reviewed all ERCP procedures performed between 08/01/2006 and 10/01/2007 by one of two experienced endoscopists (>5 years of experience) with the assistance of a trainee. Patient data was collected for indications, risk factors for PEP, type and reason for PD stent, complications, and any mortality. The PD stent was removed endoscopically if it was still in place on abdominal X-ray done 2 weeks post-ERCP. The data was analyzed with Student's t test, Chi-square, and ANOVA tests by using SPSS software version 15.0.
Results
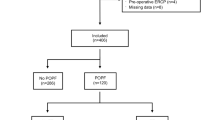
Out of a total of 753 ERCP procedures, 179 (23.8%) required either long or short prophylactic PD stents. The incidence of PEP was 3.7% versus 13.6% for long and short stent groups, respectively (p = 0.019). Spontaneous stent dislodgement rate was 95.4% versus 81.8% for long and short stent groups, respectively (p = 0.007). There was no difference in non-pancreatic complications between the two stent groups. There was no procedure-related mortality.
Conclusions
Long (>3 cm) pigtail PD stent due to their specific design showed better outcomes as compared to short (<3 cm) flanged PD stent in preventing PEP and spontaneous stent dislodgement rates. However, further prospective trials are needed.

Similar content being viewed by others


References
Tarnasky PR, Palesh YY, Cunningham JT, et al. Pancreatic stenting prevents pancreatitis after biliary sphincterotomy in patients with sphincter of Oddi dysfunction. Gastroenterology. 1998;115:1518–1524.
Smithline A, Silverman W, Rogers D, et al. Effect of prophylactic main pancreatic duct stenting on the incidence of biliary endoscopic sphincterotomy-induced pancreatitis in high-risk patients. Gastrointest Endosc. 1993;39:652–657.
Fazel A, Quadri A, Catalano MF, et al. Does a pancreatic duct stent prevent post-ERCP pancreatitis? A prospective randomized study. Gastrointest Endosc. 2003;57:291–297.
Aizawa T, Ueno N. Stent placement in the pancreatic duct prevents pancreatitis after endoscopic sphincter dilation for removal of bile duct stones. Gastrointest Endosc. 2001;34:280–285.
Sofuni A, Maguchi H, Itoi T, et al. Prophylaxis of post-endoscopic retrograde cholangiopancreatography pancreatitis by an endoscopic pancreatic spontaneous dislodgement stent. Clin Gastroenterol Hepatol. 2007;5(11):1339–1346.
Tsuchiya T, Itoi T, Sofuni A, et al. Temporary pancreatic stent to prevent post endoscopic retrograde cholangiopancreatography pancreatitis: a preliminary, single-center, randomized controlled trial. J Hepatobiliary Pancreat Surg. 2007;14(3):302–307.
Fogel EL, Eversman D, Jamidar P, et al. Sphincter of Oddi dysfunction: pancreaticobiliary sphincterotomy with pancreatic stent placement has a lower rate of pancreatitis than biliary sphincterotomy alone. Endoscopy. 2002;34:280–285.
Elton E, Howell DA, Parsons WG, et al. Endoscopic pancreatic sphincterotomy: indications, outcome, and a safe stentless technique. Gastrointest Endosc. 1998;47:240–249.
Norton ID, Gostout CJ, Baron TH, et al. Safety and outcome of endoscopic snare excision of the major duodenal papilla. Gastrointest Endosc. 2002;56:239–243.
Catalano MF, Linder JD, Chak A, et al. Endoscopic management of adenoma of the major duodenal papilla. Gastrointest Endosc. 2004;59:225–232.
Freeman ML, Overby C, Qi D. Pancreatic stent insertion: consequences of failure and results of a modified technique to maximize success. Gastrointest Endosc. 2004;5:8–14.
Vandervoort J, Soetikno RM, Montes H, et al. Accuracy and complication rate of brush cytology from bile duct versus pancreatic duct. Gastrointest Endosc. 1999;49:322–327.
Singh P, Das A, Isenberg G, et al. Does prophylactic pancreatic stent placement reduce the risk of post-ERCP acute pancreatitis: a meta-analysis of controlled trials. Gastrointest Endosc. 2004;60:544–550.
Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991;37:383–393.
Cheng CL, Sherman S, Watkins JL, et al. Risk factors for post-ERCP pancreatitis: a prospective multicenter study. Am J Gastroenterol. 2006;101:139–147.
Freeman ML, DiSario JA, Nelson DB, et al. Risk factors for post-ERCP pancreatitis: a prospective, multicenter study. Gastrointest Endosc. 2001;54:425–434.
Loperfido S, Angelini G, Benedetti G, et al. Major early complications from diagnostic and therapeutic ERCP: a prospective multicenter study. Gastrointest Endosc. 1998;48:1–10.
Masci E, Toti G, Mariani A, et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol. 2001;96:417–423.
Freeman ML, Guda NM. Prevention of post-ERCP pancreatitis: a comprehensive review. Gastrointest Endosc. 2004;59:845–864.
Sherman S, Lehman GA. ERCP and endoscopic sphincterotomy-induced pancreatitis. Pancreas. 1991;6:350–367.
Freeman ML, Nelson DB, Sherman S, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996;13:909–918.
Sherman S, Ruffolo TA, Hawes RH, et al. Complications of endoscopic sphincterotomy. A prospective series with emphasis on the increased risk associated with sphincter of Oddi dysfunction and nondilated bile ducts. Gastroenterology. 1991;101:1068–1075.
Das A, Singh P, Sivak MV Jr, et al. Pancreatic-stent placement for prevention of post-ERCP pancreatitis: a cost-effectiveness analysis. Gastrointest Endosc. 2007;65:960–968.
Somogyi L, Chuttani R, Croffie J, et al. Biliary and pancreatic stents. Gastrointest Endosc. 2006;63:910–919.
Brackbill S, Young S, Schoenfeld P, et al. A survey of physician practices on prophylactic pancreatic stents. Gastrointest Endosc. 2006;64(1):45–52.
Rashdan A, Fogel EL, McHenry L Jr, et al. Improved stent characteristics for prophylaxis of post-ERCP pancreatitis. Clin Gastroenterol Hepatol. 2004;2(4):322–329.
Guda N, Catalano MF, Geenen JE. Post ERCP pancreatitis: differences in outcomes between 3 Fr long pigtail and modified short 5 Fr Geenen stents: a randomized controlled trial. Gastrointest Endosc. 2007;65:AB113.
Chahal P, Todd HB, Tarnasky PR, et al. A prospective multicenter randomized trial of pancreatic duct stents to prevent acute post-ERCP pancreatitis. Gastrointest Endosc. 2007;65:129.
Smith MT, Sherman S, Ikenberry SO, et al. Alterations in pancreatic ductal morphology following polyethylene pancreatic stent therapy. Gastrointest Endosc. 1996;44:268–275.
Chahal P, Baron TH, Peterson BT, et al. Pancreatic stent prophylaxis of post endoscopic retrograde cholangiopancreatography pancreatitis: spontaneous migration rates and clinical outcomes. Minerva Gastroenterol Dietol. 2007;53(3):225–230.
Andriulli A, Forlano R, Napolitano G, et al. Pancreatic duct stents in the prophylaxis of pancreatic damage after endoscopic retrograde cholangiopancreatography: a systemic analysis of benefits and associated risks. Digestion. 2007;75(2–3):156–163.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Iqbal, S., Shah, S., Dhar, V. et al. Is There Any Difference in Outcomes Between Long Pigtail and Short Flanged Prophylactic Pancreatic Duct Stents?. Dig Dis Sci 56, 260–265 (2011). https://doi.org/10.1007/s10620-010-1262-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-010-1262-x