
Abstract
Purpose
Results from adjuvant trials evaluating 6 cycles of epirubicin-based chemotherapy regimens suggested these programs may be more effective than 4 cycles of doxorubicin-based chemotherapy.
Method
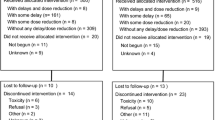
NSABP B-36 was a phase III clinical trial originally designed as a 2 × 2 factorial study comparing 6 cycles of 5-FU, epirubicin, and cyclophosphamide (FEC-100) to 4 cycles of conventional doxorubicin and cyclophosphamide (AC) with celecoxib or placebo. Shortly after activation, concerns regarding increased cardiovascular risks among selective COX-2 inhibitors resulted in a decision to remove the celecoxib/placebo from the trial. Women with histologically node-negative invasive breast cancer who had undergone primary surgery with a lumpectomy or total mastectomy were eligible. Primary endpoint was disease-free survival (DFS).
Results
Between May 2004 and July 2008, 2722 patients were enrolled. Administration of FEC-100 did not result in improvement in DFS compared to AC (HR 1.09; 95% CI 0.92–1.29, p value = 0.31). The effect of FEC-100 compared to AC on DFS was significantly different for receptor-positive (HR 1.32, 95% CI 1.05–1.66) compared to receptor-negative patients (HR 0.86, 95% CI 0.66–1.11) (treatment-by-receptor status interaction p value = 0.02). There was no statistically significant difference in the effect of treatment on overall survival (OS) with FEC-100 compared to AC (HR 1.06; 95% CI 0.84–1.35, p value = 0.61). Overall, Grade 3 and 4 adverse events were more frequent in the FEC-100 group.
Conclusion
The results of B-36 do not support use of six-cycle anthracycline-based regimens in node-negative breast cancer. Prolongation of anthracycline-based therapy with FEC-100 does not improve DFS or OS, relative to AC for 4 cycles, and was associated with expected increases in toxicity. A statistically significant interaction between treatment and hormone receptor status favoring AC in hormone-receptor-positive breast cancers is consistent with the hypothesis that optimal duration of chemotherapy may be four cycles in these patients. Late cardiac events and deaths prior to recurrence or second cancer were infrequent on both arms, but slightly higher with FEC-100.
Trial registration
ClinicalTrials.gov: NCT00087178.


Similar content being viewed by others


Change history
04 May 2022
A Correction to this paper has been published: https://doi.org/10.1007/s10549-022-06613-4
References
Fisher B, Brown AM, Dimitrov NV et al (1990) Two months of doxorubicin-cyclophosphamide with and without interval reinduction therapy compared with 6 months of cyclophosphamide, methotrexate, and fluorouracil in positive-node breast cancer patients with tamoxifen-nonresponsive tumors: results from the National Surgical Adjuvant Breast and Bowel Project B-15. J Clin Oncol 8(9):1483–1496
Fisher B, Anderson S, Tan-Chiu E et al (2001) Tamoxifen and chemotherapy for axillary node-negative, estrogen receptor-negative breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-23. J Clin Oncol 19(4):931–942. https://doi.org/10.1200/JCO.2001.19.4.931
Hutchins LF, Green SJ, Ravdin PM et al (2005) Randomized, controlled trial of cyclophosphamide, methotrexate, and fluorouracil versus cyclophosphamide, doxorubicin, and fluorouracil with and without tamoxifen for high-risk, node-negative breast cancer: treatment results of Intergroup Protocol INT-0102. J Clin Oncol 23(33):8313–8321
Levine MN, Pritchard KI, Bramwell VH et al (2005) Randomized trial comparing cyclophosphamide, epirubicin, and fluorouracil with cyclophosphamide, methotrexate, and fluorouracil in premenopausal women with node-positive breast cancer: update of National Cancer Institute of Canada Clinical Trials Group Trial MA5. J Clin Oncol 23(22):5166–5170
Fumoleau P, Kerbrat P, Romestaing P et al (2003) Randomized trial comparing six versus three cycles of epirubicin-based adjuvant chemotherapy in premenopausal, node-positive breast cancer patients: 10-year follow-up results of the French Adjuvant Study Group 01 trial. J Clin Oncol 21(2):298–305
Bonneterre J, Roché H, Kerbrat P et al (2005) Epirubicin increases long-term survival in adjuvant chemotherapy of patients with poor-prognosis, node-positive, early breast cancer: 10-year follow up results of the French Adjuvant Study Group 05 randomized trial. J Clin Oncol 23(12):2686–2693
White SJ, Freedman LS (1978) Allocation of patients to treatment groups in a controlled clinical study. Br J Cancer 37:849–857
Ganz PA, Bandos H, Geyer CE Jr, et al (2022) Behavioral and health outcomes from the NRG Oncology/NSABP B-36 trial comparing two different adjuvant therapy regimens for early-stage node-negative breast cancer. Breast Cancer Res Treat. 192(1):153–161. https://doi.org/10.1007/s10549-021-06475-2. Epub 2022 Feb 3. PMID: 35112166. https://pubmed.ncbi.nlm.nih.gov/35112166/
Lin DY, Wei LJ, Ying Z (1993) Checking the Cox model with cumulative sums of martingale-based residuals. Biometrika 80:557–572
Jacobs SA, Wilson JW, Bandos H, et al. NSABP B-36: A randomized phase III trial comparing six cycles of 5-fluorouracil (5-FU), epirubicin, and cyclophosphamide (FEC) to four cycles of adriamycin and cyclophosphamide (AC) in patients (pts) with node-negative breast cancer. Cancer Res 75 (9); SABCS 2014 December 9–13, 2015; San Antonio, TX. Abstr S3–02.
McNeil C (2000) Consensus panel endorses range of adjuvant therapies for breast cancer. J Natl Cancer Inst 92(23):1870. https://doi.org/10.1093/jnci/92.23.1870
Paik S, Tang G, Shak S et al (2006) Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol 24:3726–3734
Sparano JA, Gray RJ, Makower DF et al (2018) Adjuvant chemotherapy guided by a 21-Gene Expression Assay in breast cancer. N Engl J Med 379:111–121
Cardoso F ,van't Veer LJ (2016) Bogaerts J (2016) MINDACT Investigators: 70-Gene Signature as an aid to treatment decisions in early-stage breast cancer. N Engl J Med 375:717–729
Acknowledgements
The authors would also like to acknowledge John Wilson, PhD (retired), who was the original Protocol Statistician for the study and was an invaluable part of the protocol team. The authors acknowledge the contributions of Barbara C. Good, PhD, Director of Scientific Publications, Christine I. Rudock, Publications and Graphics Specialist, and Wendy L. Rea, BA, Editorial Associate, all of whom are employees of NSABP. They were not compensated beyond their normal salaries for this work.
Funding
This work was supported by the National Institutes of Health grants U10-CA-180868, -189867, -180822, and -44066-26; and Pharmacia & Upjohn Company, a subsidiary of Pfizer, Inc.
Author information
Authors and Affiliations
Contributions
Conceptualization: CEG Jr., HB, PR, LF, JTH, SMS, EPM, NW. Methodology: CEG Jr., HB, SMS. Software: HB. Validation: HB, EPM. Formal Analysis: HB. Investigation: CEG Jr., PR, AR, LF, PJW, JP, AMB, LP, JTH, LB-D, TBJ, SMS, HRS, EPM, NW. Resources: AR, LF, JP, AMB, AHGP, AMB, LF, LP, TBJ, EPM. Data Curation: HB, AR. Writing – Original Draft: CEG, Jr., HB, PR, SAJ, AMB, LP, JTH, SMS. Writing – Review & Editing: CEG Jr., HB, PR, LF, PJW, JP, AMB, AHGP, LP, JTH, RLC, TBJ, SMS, EPM, NW. Visualization: CEG, Jr., HB, PR, SMS, EPM. Supervision: CEG, Jr., LF, LP, EPM, NW; Project Administration: CEG, Jr., NW; Funding Acquisition: NW.
Corresponding author
Ethics declarations
Conflict of interest
Charles E. Geyer, Jr.—Grants, non-financial support and other from Genentech/Roche, Daiichi/Sankyo, and AstraZeneca, during the conduct of the study, and personal fees from Exact Sciences and Athenex, outside the submitted work. Priya Rastogi: Genentech/Roche—Unpaid advisory boards, travel, accommodations; Lilly—Travel, accommodations; Astra/Zeneca—Travel, accommodations. Johnathan Polikoff – Consultant, Natera. Louise Provencher: Consulting or Advisory Role: Lilly, Pfizer, Roche, Novartis; Research Funding: Pfizer, Roche, Novartis, Merck, GlaxoSmithKline, Odonate Therapeutics Sandra M. Swain: Personal Fees for consulting/advisory services/nonpromotional speaking: Astra-Zeneca, Athenex, Daiichi-Sankyo, Genentech/Roche, Exact Sciences (Genomic Health), Eli Lilly and Company, Bejing Medical Award Association, Merck, Natera, Molecular Templates, Silverback Therapeutics; Non-financial support (i.e., travel, accommodations, and/or food & beverage); Genentech/Roche: Research support (to institution): Genentech/Roche, Kailos Genetics; Other support: AstraZeneca (member, independent data monitoring committee) and Genentech/Roche (third-party writing assistance). Eleftherios P. Mamounas: Genentech/Roche, Exact Sciences: Consultant (Advisory Board) and Speaker’s Bureau. Biotheranostics, Daiichi Sankyo, Puma Biotechnology, Merck: Consultant (Advisory Board).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: In the original publication of the article, the word cyclophoshamide in abstract and introduction was published incorrectly. The corrected word should read as cyclophosphamide.
Supplementary Information
Below is the link to the electronic supplementary material.
10549_2021_6417_MOESM1_ESM.pdf
Subgroup analysis of disease-free survival. AC doxorubicin and cyclophosphamide, FEC-100 5-fluorouracil, epirubicin, and cyclophosphamide, HR hazard ratio, D number of events, N number of patients. Supplementary file1 (PDF 105 kb)
Rights and permissions
About this article

Cite this article
Geyer, C.E., Bandos, H., Rastogi, P. et al. Definitive results of a phase III adjuvant trial comparing six cycles of FEC-100 to four cycles of AC in women with operable node-negative breast cancer: the NSABP B-36 trial (NRG Oncology). Breast Cancer Res Treat 193, 555–564 (2022). https://doi.org/10.1007/s10549-021-06417-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-021-06417-y