
Abstract
In the United States, a context of multiple marginalization shapes sexual health disparities experienced by transgender women. Using data from 396 transgender women with negative or unknown HIV status, we performed exploratory factor analysis on responses to gender identity and sexual behavior stigma items and regressed sexual health outcomes on extracted factors via modified Poisson regression with robust variance estimation. Overall, 97.2% of participants endorsed ≥ 1 gender identity stigma; 67.2% endorsed ≥ 1 sexual behavior stigma; and 66.9% endorsed ≥ 1 of each. Extracted factors included gender-identity social stigma, reflecting experiences related to family, fearfulness in public, and verbal harassment (α = 0.68); gender-identity institutional stigma/violence, reflecting experiences related to healthcare, police interactions, and interpersonal violence (α = 0.73); and global sexual behavior stigma, reflecting experiences related to family, friends, and healthcare, as well as police interactions, fearfulness in public, verbal harassment, and interpersonal violence (α = 0.83). Gender-identity social stigma was significantly, positively associated with testing for HIV and testing for sexually transmitted infections. Gender-identity institutional stigma/violence and global sexual behavior stigma were both significantly, positively associated with condomless anal sex, sex work, testing for HIV, testing for sexually transmitted infections, and use of HIV pre-exposure prophylaxis. Stigma-mitigation remains critical to improve quality of life and sexual health for transgender women in the United States.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the United States (US), transgender women occupy social space at the intersection of multiple axes of identity—as women, as transgender people, and others (e.g., as racial/ethnic minorities)—creating potential for sexist, transphobic, and other (e.g., racist) stigma experiences across multiple contexts [1,2,3]. Stigma—an attribute of difference that discredits, devalues, and spoils one’s identity in the eyes of society [4]—can emerge via internalized (one’s own adoption of negative views toward those with the stigmatized attribute, including oneself), anticipated (expectation of mistreatment due to the stigmatized attribute), and enacted mechanisms (acts of mistreatment such as violence, discrimination, harassment, and rejection due to the stigmatized attribute) [5, 6]. Stigma not only manifests individually and interpersonally, but also communally (in norms and values that shape attitudes toward people with the stigmatized attribute) and structurally (e.g., in policies that enable denial of services or protection to people with the stigmatized attribute) [7, 8].
Gender identity stigma operates to invalidate transgender women’s lived experience and block gender-affirming resources (e.g., medical services; gender identity-matching restrooms) [7, 9]. Gender affirmation—the “interpersonal, interactive process whereby a person receives social recognition and support for their gender identity and expression” [10]—through other means (e.g., sexual behavior) could increase risk for HIV and sexually transmitted infections (STIs) [3]. As gender identity stigma can constrain socioeconomic opportunities, some transgender women may engage in sex work, conferring additional HIV/STI risk, particularly when condomless sex may yield greater financial gain [3, 11,12,13,14,15]. Gender identity stigma can constrain access to social, educational, and insurance resources, compromising health literacy and healthcare utilization, while gender identity stigma encountered in service settings may deter help-seeking [11, 16,17,18,19].
Gender identity stigma may underpin or exacerbate observed sexual health disparities among US transgender women. Meta-analytic findings indicate 21% prevalence of self-reported HIV and 14% prevalence of laboratory-confirmed HIV in this population, compared to 0.3% in the US adult population [20, 21]. Systematic reviews have found 20–25% STI prevalence among US transgender women, with > 33% engaging in recent condomless sex and participating in sex work [20, 22]. Individuals aged 13–64 years at elevated risk for HIV are advised to get tested for HIV at least yearly, though 25–61% of US transgender women have never tested for HIV, and as many as 90% have reported no past-year HIV-testing [11, 20, 23, 24]. Further, HIV pre-exposure prophylaxis (PrEP) awareness and uptake remain low [20, 25, 26].
Research has explored how intersecting gender identity and other stigmas may compound sexual health disparities for transgender women [20, 27, 28]. However, sexual behavior stigma—the shared belief system that denigrates individuals who report participation, or are perceived to participate, in non-heterosexual practices—among transgender women remains underexplored [29,30,31,32]. Transgender women may encounter sexual behavior stigma because they are misperceived as cisgender men who have sex with men, possibly due to sexual partner characteristics or because transfemininity is misperceived as male homosexuality [33]. Likewise, transgender women who have sex with women may encounter sexual behavior stigma because they identify as lesbian or bisexual or have sex with other women [11, 33].
Like gender identity stigma, sexual behavior stigma can be experienced across socioecological levels [34, 35]. While sexual behavior stigma has been linked to sexual behavior and/or healthcare utilization among transgender women in sub-Saharan Africa and in other populations in the US and elsewhere [31, 36, 37], such associations (including intersectional associations) among transgender women in the US remain unclear. Intersectionality posits that social identities/positions and social inequality share an interdependent and mutually constitutive relationship [38]. While stigma related to gender identity and sexual behavior may be linked to transgender women’s sexual health in distinct ways, they may also intersect synergistically. Moreover, each stigma may operate or be experienced differently across other identities and social positions, such as race/ethnicity and age [20, 27, 28, 39,40,41,42,43,44,45,46].
The Present Study
The purpose of this study was to assess gender identity and sexual behavior stigma and determine independent and intersectional associations with sexual health outcomes—including condomless anal and vaginal sex, sex work, HIV and STI testing, and PrEP use—in an online sample of US transgender women. The focus on stigma experiences and potential associations with sexual health does not negate the fact that transgender women possess agency and demonstrate strength and resilience in stigmatizing contexts [47,48,49].
Minority stress theories and the gender affirmation framework [3, 50,51,52,53,54], as well as previous research, informed our hypotheses. First, we expected that gender identity and sexual behavior stigma would be positively associated with condomless sex and sex work, as invalidation of gender identity may lead to alternative avenues for affirmation, such as condomless sex [3], and stigmatization of identity may constrain socioeconomic opportunities, leading to sex work [11, 13]. Moreover, gender-related and sexuality-based stigma have both been found to be positively associated with condomless anal sex and sex work participation among transgender women in prior research [37, 55,56,57].
We hypothesized that gender identity and sexual behavior stigma would be associated with each sexual health service utilization outcome, but given mixed findings/associations in prior research, we did not specify directionality. For example, minority stress and gender affirmation models would posit stigma as a barrier to accessing sexual health services [3, 50,51,52, 54], which has been demonstrated previously [26, 56,57,58,59]. However, some transgender women may endure stigma as part of the healthcare experience [56, 60], or experience both stigma and gender affirmation when utilizing healthcare, with gender affirmation mitigating the effects of ongoing stigma and facilitating further healthcare [61].
Lastly, informed by intersectionality [38, 62], we expected the co-existence of both gender identity and sexual behavior stigma to amplify stigma-outcome associations [29, 63]. Additionally, given enhanced vulnerabilities among young transgender women and transgender women of Color, including syndemic factors (e.g., violence and other forms of victimization, substance use) and high HIV and STI prevalence [12, 20, 29, 40, 64, 65], we expected stigma-outcome associations to be stronger among younger and racial/ethnic minority participants.
Methods
Data, Participants, and Procedures
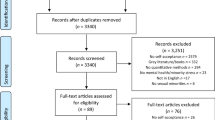
Methods on the Transgender Women’s Internet Survey and Testing (TWIST) study have been described elsewhere [66]. Briefly, participants were recruited through online convenience sampling using banner advertisements on mobile dating applications (e.g., Grindr) and social media platforms (e.g., Facebook) from March–April 2019. Eligibility criteria included age ≥ 15 years, self-identification as a transgender woman or transfeminine person, self-report of a valid US ZIP code, and ever having had oral, anal, or vaginal sex. There were no HIV status-related criteria or restrictions on participation, but we were interested in examining stigma’s association with sexual health among those who were not knowingly living with HIV. Participants ≥ 18 years provided online informed consent, and participants 15–17 years provided online informed assent (parental consent waived by institutional review board) before beginning the online survey in English using SurveyGizmo (Boulder, CO, USA). No incentive was provided. The original study was approved by Emory University Institutional Review Board, and this secondary analysis of deidentified data was deemed exempt from review by Johns Hopkins University Institutional Review Board.
Measures
Participants responded to 1 set of 13 sexual behavior stigma items and 1 set of 13 gender identity stigma items, which served as independent variables (Table 1). Items were based on a set of sexual behavior stigma items originally developed to measure sexual behavior stigma affecting cisgender men who have sex with men [67,68,69,70,71,72,73]. While a limitation that the items were not originally developed with transgender women, the adaptation of these items was significant, including consultations with transgender researchers and a community advisory board comprised of transgender women. Collectively, the goal of the adaptation process was to better ensure that these items were representative of transgender women's lived experience and to ensure their adaptation for use with transgender women.
Stigma items assessed perceptions, anticipations, and experiences of gender identity and sexual behavior stigma in social, healthcare, and other contexts. Though several of the stigma items reflect experiences that were conceptualized and categorized as “perceived” stigma a priori during the scale development process (e.g., "Have you ever felt excluded from family activities because of your gender identity?”), these experiences certainly could have been objective instances of mistreatment (i.e., enacted stigma). Response options included “no,” “yes, in the past 6 months,” and “yes, but not in the past 6 months.” For analysis, responses were dichotomized by collapsing the affirmative responses to create lifetime experience of stigma versus none. For items 12 (experienced physical violence) and 13 (experienced sexual violence), participants were first asked if they experienced the violence, and if yes, they were asked if the violence was due to their gender identity or sexual behavior. Endorsement of both the experience of violence and attribution to gender identity (or sexual behavior) were coded “yes.”
We examined several past-year sexual health outcomes with yes/no items: condomless anal sex (insertive/receptive), condomless vaginal sex (insertive/receptive), sex work (was given drugs or money in exchange for sex), HIV testing, STI testing (gonorrhea, chlamydia, or syphilis), and PrEP use. Narrower or more recent timeframes were not assessed because, like its predecessor (the American Men’s Internet Survey [AMIS; [74, 75]]), TWIST was designed to assess and monitor broader, yearly trends in HIV-relevant behaviors and healthcare utilization [66]. Covariates included age in years, education (high school education or less; some college, associate’s degree, or technical school; college graduate or graduate school), race/ethnicity (non-Hispanic white, non-Hispanic Black, non-Hispanic Multiracial and Other Races, Hispanic), sexual identity (homosexual or gay, heterosexual or straight, bisexual or pansexual, queer, or other, including asexual, questioning, or another identity), insurance status (uninsured or not), and urbanicity (large metro, suburban, small/medium metro, and rural).
Analysis
Frequencies were calculated for endorsement of stigma items, and exploratory factor analysis (EFA) was performed separately on each item set to characterize stigma burden through detection of underlying constructs.
Specifically, a tetrachoric correlation matrix was generated given dichotomous response options, upon which a principal components analysis was performed. Next, the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy was calculated to determine the data’s suitability for factor analysis [76, 77]. A scree plot was subsequently generated, and a parallel analysis was performed to reveal potential factor solutions, upon which EFA with robust weighted least squares estimation (to avoid convergence problems) was performed [78]. An oblique-quartimin rotation was applied due to expected inter-factor correlations and to minimize variable complexity [79, 80]. Loadings ≥ 0.40 that did not cross-load were retained [81]. Model selection was based on the number of strongly loading factors, parsimony, and scientific interpretation. Cronbach’s alphas were calculated to determine the internal consistency of extracted factors.
Descriptive statistics were calculated for sociodemographic characteristics and outcome variables. Mean factor scores were calculated by summing the number of endorsed stigma experiences per factor, dividing by the number of non-missing items, and rescaling by a factor of 10 to improve interpretability. Chi-squared and Kruskal–Wallis tests were used to assess outcome differences in sociodemographic characteristics and stigma factor scores; for significant chi-squared tests involving sociodemographic characteristics comprised of more than two groups, adjusted residuals were calculated to determine which specific subgroup(s) proportions significantly differed across each outcome. Bivariate modified Poisson regressions with robust variance estimation were performed between each outcome and stigma factor [82]. Multivariable regressions were performed for each independent variable that had a bivariate association (p < 0.10) with a given outcome.
To examine the extent to which stigmas intersected on outcomes [63], we added two-way product terms between mean-centered sexual behavior and gender identity stigma factors [83]. We also tested two-way product terms between age (dichotomized at median) and each stigma factor, and between race/ethnicity (racial/ethnic minorities versus non-Hispanic white) and each stigma factor [63]. Coefficients were exponentiated to generate prevalence ratios. Wald tests, with statistical significance set at p < 0.05, and 95% confidence intervals (CI) were calculated and examined. Analyses were conducted in Stata Version 15 [84] and Mplus Version 8 [78].
Results
Sample Characteristics
A total of 401 participants completed the survey, 5 (1.2%) of whom reported living with HIV and were therefore outside the scope of interest for this study. We excluded these participants, leaving 396 with HIV-negative or unknown status. Roughly 1 in 3 were from the South, and median age was 24 years. Over 70% were non-Hispanic white, and 44.9% identified as bisexual or pansexual (Table 2). In the past year, 28.3% (112/396) reported condomless anal sex, 32.3% (128/396) reported condomless vaginal sex, 7.3% (29/396) reported sex work, 36.6% (145/396) had been tested for HIV, 31.8% (126/396) had been tested for STIs, and 5.6% (22/396) had used PrEP.
Condomless anal sex was associated with heterosexual/straight identity (χ2 = 12.14[4], p < 0.05), and condomless vaginal sex was associated with having earned a college degree or more (χ2 = 12.27[2], p < 0.01). Sex work was associated with non-Hispanic Black and Hispanic race/ethnicity (χ2 = 24.39[3], p < 0.001) and heterosexual/straight identity (χ2 = 13.51[4], p < 0.01). HIV testing was associated with older age (χ2 = 14.20[1], p < 0.05) and having earned a college degree or more (χ2 = 16.03[2], p < 0.001). STI testing was associated with having earned a college degree or more (χ2 = 11.81[2], p < 0.01), queer identity (χ2 = 10.11[4], p < 0.05), having insurance (χ2 = 4.28[1], p < 0.05), and residing in a large metro area (χ2 = 9.01[3], p < 0.05). PrEP use was associated with heterosexual/straight identity (χ2 = 14.18[4], p < 0.01), residing in a large metro area (χ2 = 10.25[3], p < 0.05), and residing in the West (χ2 = 8.64[3], p < 0.05). Additional associations are noted in Table 3.
Gender Identity Stigma
Of the 13 gender identity stigma experiences assessed, respondents endorsed an average of 6.0 experiences, with 97.2% (385/396) endorsing ≥ 1 and 93.4% (370/396) endorsing ≥ 2. The most endorsed experience was feeling afraid in public (340/396, 85.9%), followed by verbal harassment (75.3%), exclusion from family activities (74.0%), and family gossip/discriminatory remarks (73.7%; Table 1). A two-factor model best fit the data. Factor 1 consisted of 4 items related to family, fearfulness in public, and verbal harassment and was named “gender-identity social stigma” (α = 0.68). Factor 2 consisted of 5 items related to healthcare, police interactions, and interpersonal violence and was named “gender-identity institutional stigma/violence” (α = 0.73). These factors were moderately correlated (r = 0.52). Other items were removed due to high correlations with other items, low KMO values, or low loadings.
Participants reporting greater gender-identity social stigma were significantly more likely to report HIV (aPR = 1.08, 95% CI 1.02, 1.15) and STI testing (aPR = 1.13, 95% CI 1.05, 1.22). Those reporting greater gender-identity institutional stigma/violence were significantly more likely to report condomless anal sex (aPR = 1.07, 95% CI 1.02, 1.13), sex work (aPR = 1.31, 95% CI 1.13, 1.52), HIV testing (aPR = 1.07, 95% CI 1.03, 1.11), STI testing (aPR = 1.07, 95% CI 1.03, 1.11), and PrEP use (aPR = 1.17, 95% CI 1.01, 1.34) (Table 4).
Sexual Behavior Stigma
Of the 13 sexual behavior stigma experiences assessed, respondents endorsed an average of 2.5 stigma experiences, with 67.2% (266/396) endorsing ≥ 1 and 50.8% (201/396) endorsing ≥ 2. The most endorsed sexual behavior stigma experience was verbal harassment (37.6%), followed by gossip/discriminatory remarks by family (36.9%) and feeling afraid in public (33.1%; Table 1). A one-factor model comprised of nine items, all of which loaded > 0.60, best fit the data, and the factor was named “global sexual behavior stigma” (α = 0.83). Other items were removed due to low endorsement (< 11%) that prohibited conducting principal components analysis. Participants reporting greater sexual behavior stigma were significantly more likely to report condomless anal sex (aPR = 1.10, 95% CI 1.05, 1.16), sex work (aPR = 1.37, 95% CI 1.16, 1.61), HIV testing (aPR = 1.07, 95% CI 1.03, 1.12), STI testing (aPR = 1.08, 95% CI 1.04, 1.13), and PrEP use (aPR = 1.24, 95% CI 1.07, 1.43) (Table 4).
Product Terms
Roughly two thirds of participants (265/396, 66.9%) endorsed ≥ 1 gender identity and ≥ 1 sexual behavior stigma, and 50.0% (198/396) endorsed ≥ 2 of each. The product term for gender-identity social stigma and gender-identity institutional stigma/violence on condomless vaginal sex was significant in multivariable analyses (p = 0.004). Simple slopes for gender-identity social stigma were significant at all values (1–10) of gender-identity institutional stigma/violence (all p < 0.05; Fig. 1). In other words, the marginal effect of gender-identity social stigma on condomless vaginal sex depended on the extent of gender-identity institutional stigma/violence experienced, with a more consequential effect (i.e., greater risk for condomless vaginal sex) the higher the gender-identity institutional stigma/violence. The adjusted effect remained significant (p = 0.011) when restricted to participants who had not had gender affirmation surgery (n = 376, 95.0%), and all simple slopes of gender-identity social stigma remained significant (p < 0.05) at each value of gender-identity institutional stigma/violence except when the value was 1 (p = 0.086; not shown). No other product terms were significant (not shown).

Average marginal effects of gender-identity social stigma (with 95% confidence intervals [CIs]) on condomless vaginal sex at all possible values of gender-identity institutional stigma/violence among transgender women in the United States
Discussion
In this study, we identified latent constructs of gender identity stigma, including gender-identity social stigma and gender-identity institutional stigma/violence, with borderline adequate and adequate internal consistency, respectively. We also identified an underlying construct of sexual behavior stigma—global sexual behavior stigma—which had adequate internal consistency. We found a high burden of each stigma subtype across participants, and we documented associations between each latent stigma construct and several sexual health outcomes, including sexual behaviors, sex work, and sexual health service utilization.
Our findings are consistent with research that has documented high prevalence of gender identity stigma among transgender women in diverse settings [11, 16]. We extend these findings by also showing a high burden of sexual behavior stigma, justifying calls for the inclusion of sexuality-based stigma in research and intervention-development with this population [29, 85]. Among the most endorsed stigma experiences across gender identity and sexual behavior were fear when in public and verbal harassment. Transphobic verbal harassment is commonplace for many transgender women [86, 87], which, in conjunction with structural (e.g., bathroom bills, sports bans) and interpersonal violence (e.g., assault, murder) against the transgender community, could conceivably foster a sense of threat and fear when in public spaces [88,89,90,91,92]. Additional threats of harm based on sexual prejudice may exacerbate this sense and lead to verbal harassment in even more contexts.
Gender-identity social stigma featured perceived/enacted negative interactions with others and fear when in situations (i.e., in public) that may facilitate such interactions. What drove the constitution of this factor is unclear, as different forms of stigma (anticipated, perceived/enacted) in diverse contexts (family, public, unspecified) were represented. Gender-identity institutional stigma/violence featured negative encounters with healthcare and legal institutions, and physically and sexually violent interpersonal encounters. Form and context may have driven this factor’s composition, as several items pertained to perceived/enacted stigma. Moreover, institutional stigma was represented in several of the items, while violence was represented in the others.
Sexual behavior stigma featured a mix of social and institutional stigma and violence. Item-removal driven by low endorsement may have prevented detection of additional constructs underlying sexual behavior stigma items [93], though one construct may in fact best represent experiences of sexual behavior stigma for transgender women in our sample; this is an area for future research. Notably, several healthcare stigma items were among the least-endorsed, possibly indicating that stigmatization in healthcare contexts is experienced as gender identity- rather than sexuality-related, or that providers and transgender women rarely discuss sex. Transgender women may consider sexual behavior issues less relevant to their healthcare, or providers may lack competence to address gender minorities’ sexual health [94, 95].
Though comprised of the most commonly endorsed experiences, gender-identity social stigma was associated with past-year HIV and STI testing only. Prior research has linked gender identity and other types of stigma to transgender women’s sexual health service utilization, as both a reason to delay sexual health services and as an unavoidable component of receiving them [60, 96], either of which could explain our findings. This relationship could also be explained by disclosure, with individuals who utilize sexual health services being likely to disclose their gender identity as part of the healthcare assessment, experiencing stigma as a result.
Though comprised of the least commonly endorsed stigma experiences, gender-identity institutional stigma/violence was associated with nearly all examined outcomes: condomless anal sex, sex work, HIV and STI testing, and PrEP use. Sex work contexts may more easily facilitate gender identity stigmatization or even victimization by both police/legal systems and sex work clients [15], while healthcare contexts may facilitate stigmatization when attempting to access sexual health services. Moreover, stigma in the form of denial of gender-affirming services or transphobic violence may exacerbate the need for gender affirmation while also restricting accessible avenues for it, which could lead to engagement in sexual behaviors to secure gender affirmation [3].
Like gender identity institutional stigma/violence, global sexual behavior stigma had strong associations with sexual behaviors, sex work, and sexual health service utilization. While transgender women may encounter sexual behavior stigma due to sexual identity, sexual partner characteristics, or misperceptions about their gender identity [11, 33, 97], they may also encounter sexual behavior stigma because sexual practices such as condomless anal sex and occupations such as sex work are stigmatized [31, 97,98,99,100]. The reverse has also been shown, wherein experiences of stigma due to one’s presumed sexual behavior or sexuality may lead to participation in these practices [101, 102]. Likewise, sexual health service utilization typically requires disclosure of one’s sexual behaviors or other sexuality-based attributes to healthcare workers, which may also lead to stigmatization [103, 104]. Further, sexual health service utilization, particularly PrEP use, is often conflated with stigmatized sexual behavior [105]. Incorporating a sex-positive perspective into medical/public health discourse could be effective for both sexual behavior stigma-mitigation and sexuality-affirmation in this population.
That our gender identity-by-sexual behavior product terms were non-significant does not negate the fact that these are intersecting attributes or that they may lead to intersecting stigma experiences. The lack of findings could reflect how these stigmas operate uniquely and independently of one another for this sample of transgender women, but could also reflect selective stigmatization and differences in disclosure across contexts (or participants’ being asked to report their experiences of stigma separately by stigmatized identity/attribute). A lack of statistical power and the relative homogeneity of the sample (thereby limiting the diversity of potential experiences of both stigmas) could have contributed as well.
However, we did find that gender-identity social and institutional stigma/violence interacted to increase risk for condomless vaginal sex. For transgender women who have not had or who do not want gender affirmation surgery, condomless vaginal sex can potentiate HIV risk, and though under-researched, prior studies have linked transgender women’s engagement in condomless vaginal sex to HIV/STI risk [55]. Such a substantial burden of both gender-identity social and institutional stigma/violence may be particularly isolating, in terms of both social and material resources, resulting in restricted access to safe sex tools or fostering a need for intimacy and connection that may be achieved through condomless sex. Condomless sex may act as an avoidant, albeit useful, strategy to cope with stigma, serving as an escape from any thoughts or emotions resulting from that stigma [106,107,108]. Notably, prior research has documented greater distress and greater use of avoidant coping among transgender persons who have less social support or who are earlier in the transition or affirmation process [109]. Identifying mechanisms linking gender-identity social and institutional stigma/violence to condomless vaginal sex merits future research.
Our findings echo the need for structural- and community-level interventions to mitigate stigma, affirm gender identity and sexuality, and increase safe, equitable access to socioeconomic (including housing, education, and employment), healthcare, and other resources. While recent legislation (such as the Bostock v. Clayton County ruling, which provided federal protection for employees against discrimination because they are transgender or a sexual minority) could somewhat aid in these efforts [110, 111], other ongoing legislation (e.g., bathroom bills, sports participation restrictions, gender affirmation care bans, bans of books and classroom discussions pertaining to sexuality and gender, and the like) rooted in status-quo oppressive power structures (e.g., sexism and cisgenderism, heteropatriarchy, white supremacy, capitalism) will continue to undermine them, constraining the human rights of and increasing stigma toward transgender people, exacerbating social and health inequities further [88, 112]. Collective and concerted efforts remain warranted to identify and disrupt intersectional causes of transgender health inequities, including structures of domination that shape institutional systems and socio-cultural processes [113].
Limitations
Findings should be considered in light of limitations. First, as this was an online convenience sample of young, mostly non-Hispanic white transgender women, results may not be generalizable to more diverse samples unlikely to be recruited online. Further, these sample characteristics, especially the lack of racial/ethnic diversity, limit the extent to which our findings can richly contribute to understandings of HIV-related health inequities. Second, the small sample size and even smaller cell values of some subgroups prevented modeling and possibly the detection of some relationships. Third, the data were cross-sectional, preventing the establishment of temporality. Future qualitative research to understand better the directionality of the relationships found here, particularly the relationships with sexual health testing and PrEP use, would be useful. Relatedly, the recall period for all outcomes was the 12 months prior to survey completion, which could have resulted in recall bias. Fifth, stigma items removed in preliminary analyses were not subjected to EFA. Items may behave differently in larger, more diverse samples and not necessitate removal, yielding an alternative factor structure. Removal may also indicate the need for more refinement of some items. Incentives were not provided for completing the survey, which may have discouraged some individuals from participation. Finally, we examined self-reported stigma experiences perceived to be related to one’s gender identity and sexual behavior, requiring some level of subjective judgment and therefore possible bias.
Conclusion
Results of this study highlight the multifaceted burden of gender identity and sexual behavior stigma encountered by US transgender women and stigma’s complex linkages to sexual health. Stigma-mitigation interventions must be more innovative and intentional in targeting the socio-environmental contexts (e.g., family, healthcare) in which stigma emerges or is experienced. With COVID-19 constraining healthcare access further, addressing stigma may be even more consequential for preventing the exacerbation of sexual health disparities. Understanding that sexuality is part of transgender women’s lived experience and ensuring that sexuality is integrated into gender identity stigma-mitigation interventions for transgender women across settings, including programs that train providers in transgender-competent care, will be key in these efforts.
Data Availability
The data are not publicly available to protect confidentiality. Requests to access the data should be send to authors SDB and THS.
Code Availability
Code may be made available by contacting the first author.
References
Butler J. Gender trouble: feminism and the subversion of identity. New York: Routledge; 1990.
Serano J. Whipping girl: a transsexual woman on sexism and the scapegoating of femininity. Emeryville: Seal Press; 2007.
Sevelius JM. Gender affirmation: a framework for conceptualizing risk behavior among transgender women of color. Sex Roles. 2013;68(11–12):675–89.
Goffman E. Stigma: Notes on the management of spoiled identity. New York: Simon & Schuster; 1963.
Earnshaw VA, Chaudoir SR. From conceptualizing to measuring HIV stigma: a review of HIV stigma mechanism measures. AIDS Behav. 2009;13(6):1160–77.
Turan B, Budhwani H, Fazeli PL, Browning WR, Raper JL, Mugavero MJ, et al. How does stigma affect people living with HIV? The Mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS Behav. 2017;21(1):283–91.
White Hughto JM, Reisner SL, Pachankis JE. Transgender stigma and health: a critical review of stigma determinants, mechanisms, and interventions. Soc Sci Med. 2015;147:222–31.
Poteat TC, Logie CH, Adams D, Mothopeng T, Lebona J, Letsie P, et al. Stigma, sexual health, and human rights among women who have sex with women in Lesotho. Reprod Health Matters. 2015;23(46):107–16.
Hendricks ML, Testa RJ. A conceptual framework for clinical work with transgender and gender nonconforming clients: an adaptation of the minority stress model. Prof Psychol Res Pract. 2012;43(5):460–7.
Jae S, Valerie J. Challenges and opportunities for gender-affirming healthcare for transgender women in prison. Int J Prisoner Health. 2017;13(1):32–40.
James S, Herman J, Rankin S, Keisling M, Mottet L, Anafi M. The report of the 2015 US transgender survey. 2016.
Baral SD, Poteat T, Stromdahl S, Wirtz AL, Guadamuz TE, Beyrer C. Worldwide burden of HIV in transgender women: a systematic review and meta-analysis. Lancet Infect Dis. 2013;13(3):214–22.
Poteat T, Reisner SL, Radix A. HIV epidemics among transgender women. Curr Opin HIV AIDS. 2014;9(2):168–73.
Reisner SL, Mimiaga MJ, Bland S, Mayer KH, Perkovich B, Safren SA. HIV risk and social networks among male-to-female transgender sex workers in Boston, Massachusetts. J Assoc Nurses AIDS Care. 2009;20(5):373–86.
Sausa LA, Keatley J, Operario D. Perceived risks and benefits of sex work among transgender women of color in San Francisco. Arch Sex Behav. 2007;36(6):768–77.
Grant J, Mottet L, Tanis J, Harrison J, Herman J, Keisling M. Injustice at every turn: A report of the National Transgender Discrimination Survey. 2011.
Gonzales G, Henning-Smith C. Barriers to care among transgender and gender nonconforming adults. Milbank Q. 2017;95(4):726–48.
United Nations Development Programme [UNDP]. Discussion paper: Transgender health and human rights. 2013.
United Nations Development Programme, IRGT: A Global Network of Transgender Women and HIV, United Nations Population Fund, UCSF Center of Excellence for Transgender Health, Johns Hopkins Bloomberg School of Public Health, World Health Organization, Joint United Nations Programme on HIV/AIDS, United States Agency for International Development [UNDP]. Implementing comprehensive HIV and STI programmes with transgender people: Practical guidance for collaborative interventions. 2016.
Becasen JS, Denard CL, Mullins MM, Higa DH, Sipe TA. Estimating the prevalence of HIV and sexual behaviors among the US transgender population: a systematic review and meta-analysis, 2006–2017. Am J Public Health. 2018;29:e1–8.
Centers for Disease Control and Prevention. HIV Surveillance Report: Diagnoses of HIV Infection in the United States and dependent areas, 2020 (updated). 2021;33.
Dewart CM, Bernstein KT, DeGroote NP, Romaguera R, Turner AN. Prevalence of rectal chlamydial and gonococcal infections: a systematic review. Sex Transm Dis. 2018;45(5):287–93.
Pitasi MA, Oraka E, Clark H, Town M, DiNenno EA. HIV testing among transgender women and men-27 states and Guam, 2014–2015. MMWR Morb Mortal Wkly Rep. 2017;66(33):883–7.
Downing JM, Przedworski JM. Health of transgender adults in the US, 2014–2016. Am J Prev Med. 2018;55(3):336–44.
Pacifico de Carvalho N, Mendicino CCP, Candido RCF, Alecrim DJD, Menezes de Padua CA. HIV pre-exposure prophylaxis (PrEP) awareness and acceptability among trans women: a review. AIDS Care. 2019;31(10):1234–40.
Vaitses Fontanari AM, Zanella GI, Feijo M, Churchill S, Rodrigues Lobato MI, Costa AB. HIV-related care for transgender people: a systematic review of studies from around the world. Soc Sci Med. 2019;230:280–94.
Herbst JH, Jacobs ED, Finlayson TJ, McKleroy VS, Neumann MS, Crepaz N, et al. Estimating HIV prevalence and risk behaviors of transgender persons in the United States: a systematic review. AIDS Behav. 2008;12(1):1–17.
Logie CH, James L, Tharao W, Loutfy MR. HIV, gender, race, sexual orientation, and sex work: a qualitative study of intersectional stigma experienced by HIV-positive women in Ontario, Canada. PLoS Med. 2011;8(11): e1001124.
Lacombe-Duncan A. An intersectional perspective on access to HIV-related healthcare for transgender women. Transgend Health. 2016;1(1):137–41.
Herek GM. Sexual stigma and sexual prejudice in the United States: a conceptual framework. Nebr Symp Motiv. 2009;54:65–111.
Fitzgerald-Husek A, Van Wert MJ, Ewing WF, Grosso AL, Holland CE, Katterl R, et al. Measuring stigma affecting sex workers (SW) and men who have sex with men (MSM): a systematic review. PLoS ONE. 2017;12(11): e0188393.
Herek G, Chopp R, Strohl D. Sexual stigma: putting sexual minority health issues in context. In: Meyer I, Northridge M, editors. The health of sexual minorities: public health perspectives on lesbian, gay, bisexual, and transgender populations. Boston: Springer; 2007. p. 171–208.
Mizock L, Hopwood R. Conflation and interdependence in the intersection of gender and sexuality among transgender individuals. Psychol Sex Orientat Gend Divers. 2016;3(1):93–103.
Baral S, Logie CH, Grosso A, Wirtz AL, Beyrer C. Modified social ecological model: a tool to guide the assessment of the risks and risk contexts of HIV epidemics. BMC Public Health. 2013;13:482.
Herek GM. Confronting sexual stigma and prejudice: theory and practice. J Soc Iss. 2007;63(4):905–25.
Arreola S, Santos GM, Beck J, Sundararaj M, Wilson PA, Hebert P, et al. Sexual stigma, criminalization, investment, and access to HIV services among men who have sex with men worldwide. AIDS Behav. 2015;19(2):227–34.
Stahlman S, Liestman B, Ketende S, Kouanda S, Ky-Zerbo O, Lougue M, et al. Characterizing the HIV risks and potential pathways to HIV infection among transgender women in Cote d’Ivoire, Togo and Burkina Faso. J Int AIDS Soc. 2016;19(3 Suppl 2):20774.
Bowleg L. When Black + Lesbian + Woman ≠ Black Lesbian woman: the methodological challenges of qualitative and quantitative intersectionality research. Sex Roles. 2008;59(5):312–25.
Garofalo R, Deleon J, Osmer E, Doll M, Harper GW. Overlooked, misunderstood and at-risk: exploring the lives and HIV risk of ethnic minority male-to-female transgender youth. J Adolesc Health. 2006;38(3):230–6.
Garofalo R, Kuhns LM, Reisner SL, Mimiaga MJ. Behavioral interventions to prevent HIV transmission and acquisition for transgender women: a critical review. J Acquir Immune Defic Syndr. 2016;15(72 Suppl 3):S220–5.
Wilson E, Chen YH, Pomart WA, Arayasirikul S. Awareness, interest, and HIV pre-exposure prophylaxis candidacy among young transwomen. AIDS Patient Care STDS. 2016;30(4):147–50.
Wilson EC, Garofalo R, Harris RD, Herrick A, Martinez M, Martinez J, et al. Transgender female youth and sex work: HIV risk and a comparison of life factors related to engagement in sex work. AIDS Behav. 2009;13(5):902–13.
Wilson EC, Chen YH, Arayasirikul S, Fisher M, Pomart WA, Le V, et al. Differential HIV risk for racial/ethnic minority trans*female youths and socioeconomic disparities in housing, residential stability, and education. Am J Public Health. 2015;105(Suppl 3):e41–7.
Poteat T, Scheim A, Xavier J, Reisner S, Baral S. Global epidemiology of HIV infection and related syndemics affecting transgender people. J Acquir Immune Defic Syndr. 2016;72(Suppl 3):S210–9.
Kuhns LM, Reisner SL, Mimiaga MJ, Gayles T, Shelendich M, Garofalo R. Correlates of PrEP indication in a multi-site cohort of young HIV-uninfected transgender women. AIDS Behav. 2016;20(7):1470–7.
Brennan J, Kuhns LM, Johnson AK, Belzer M, Wilson EC, Garofalo R, et al. Syndemic theory and HIV-related risk among young transgender women: the role of multiple, co-occurring health problems and social marginalization. Am J Public Health. 2012;102(9):1751–7.
Lacombe-Duncan A, Logie CH, Newman PA, Bauer GR, Kazemi M. A qualitative study of resilience among transgender women living with HIV in response to stigma in healthcare. AIDS Care. 2020;32(8):1008–13.
Rouhani S, Decker MR, Tomko C, Silberzahn B, Allen ST, Park JN, et al. Resilience among cisgender and transgender women in street-based sex work in Baltimore, Maryland. Womens Health Issues. 2021;31(2):148–56.
Sun CJ, Anderson KM, Mayer L, Kuhn T, Klein CH. Findings from formative research to develop a strength-based HIV prevention and sexual health promotion mHealth intervention for transgender women. Transgend Health. 2019;4(1):350–8.
Meyer IH. Minority stress and mental health in gay men. J Health Soc Behav. 1995;36(1):38–56.
Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull. 2003;129(5):674–97.
Lefevor GT, Boyd-Rogers C, Sprague BM, Janis RA. Health disparities between genderqueer, transgender, and cisgender individuals: an extension of minority stress theory. J Couns Psychol. 2019;66(4):385–95.
Testa RJ, Michaels MS, Bliss W, Rogers ML, Balsam KF, Joiner T. Suicidal ideation in transgender people: gender minority stress and interpersonal theory factors. J Abnorm Psychol. 2017;126(1):125–36.
Testa RJ, Habarth J, Peta J, Balsam K, Bockting W. Development of the gender minority stress and resilience measure. Psychol Sex Orientat Gend Divers. 2015;2(1):65–77.
Nemoto T, Bödeker B, Iwamoto M, Sakata M. Practices of receptive and insertive anal sex among transgender women in relation to partner types, sociocultural factors, and background variables. AIDS Care. 2014;26(4):434–40.
Magno L, Silva, Veras MA, Pereira-Santos M, Dourado I. Stigma and discrimination related to gender identity and vulnerability to HIV/AIDS among transgender women: a systematic review. Cad Saude Publica. 2019;35(4):e00112718.
Aggarwal NK, Consavage KE, Dhanuka I, Clement KW, Bouey JH. Health and health care access barriers among transgender women engaged in sex work: a synthesis of U.S.-based studies published 2005–2019. LGBT Health. 2021;8(1):11–25.
Dang M, Scheim AI, Teti M, Quinn KG, Zarwell M, Petroll AE, et al. Barriers and facilitators to HIV pre-exposure prophylaxis uptake, adherence, and persistence among transgender populations in the United States: a systematic review. AIDS Patient Care STDS. 2022;36(6):236–48.
Rosenberg S, Callander D, Holt M, Duck-Chong L, Pony M, Cornelisse V, et al. Cisgenderism and transphobia in sexual health care and associations with testing for HIV and other sexually transmitted infections: Findings from the Australian Trans & Gender Diverse Sexual Health Survey. PLoS ONE. 2021;16(7): e0253589.
Sevelius JM, Patouhas E, Keatley JG, Johnson MO. Barriers and facilitators to engagement and retention in care among transgender women living with human immunodeficiency virus. Ann Behav Med. 2014;47(1):5–16.
Goldenberg T, Jadwin-Cakmak L, Popoff E, Reisner SL, Campbell BA, Harper GW. Stigma, gender affirmation, and primary healthcare use among black transgender youth. J Adolesc Health. 2019;65(4):483–90.
Crenshaw KW. Mapping the margins: Intersectionality, identity, and violence against women of color. Standford Law Rev. 1991;43(6):1241–300.
Turan JM, Elafros MA, Logie CH, Banik S, Turan B, Crockett KB, et al. Challenges and opportunities in examining and addressing intersectional stigma and health. BMC Med. 2019;17(1):7.
Reisner SL, Greytak EA, Parsons JT, Ybarra ML. Gender minority social stress in adolescence: disparities in adolescent bullying and substance use by gender identity. J Sex Res. 2015;52(3):243–56.
Clark H, Babu AS, Wiewel EW, Opoku J, Crepaz N. Diagnosed HIV infection in transgender adults and adolescents: results from the National HIV Surveillance System, 2009–2014. AIDS Behav. 2017;21(9):2774–83.
Zlotorzynska M, Sanchez T, Scheim A, Lyons C, Maksut J, Wiginton J, et al. Transgender Women's Internet Survey and Testing: Protocol and Key Indicators Report. Transgender Health 2020.
Baral S, Burrell E, Scheibe A, Brown B, Beyrer C, Bekker LG. HIV risk and associations of HIV infection among men who have sex with men in peri-urban Cape Town, South Africa. BMC Public Health. 2011;11:766.
Baral S, Trapence G, Motimedi F, Umar E, Iipinge S, Dausab F, et al. HIV prevalence, risks for HIV infection, and human rights among men who have sex with men (MSM) in Malawi, Namibia, and Botswana. PLoS ONE. 2009;4(3): e4997.
Poteat T, Diouf D, Drame FM, Ndaw M, Traore C, Dhaliwal M, et al. HIV risk among MSM in Senegal: a qualitative rapid assessment of the impact of enforcing laws that criminalize same sex practices. PLoS ONE. 2011;6(12): e28760.
Dramé FM, Peitzmeier S, Lopes M, Ndaw M, Sow A, Diouf D, et al. Gay men and other men who have sex with men in West Africa: evidence from the field. Cult Health Sex. 2013;15(Suppl):7–21.
Kennedy CE, Baral SD, Fielding-Miller R, Adams D, Dludlu P, Sithole B, et al. “They are human beings, they are Swazi”: intersecting stigmas and the positive health, dignity and prevention needs of HIV-positive men who have sex with men in Swaziland. J Int AIDS Soc. 2013;16:18749.
Cange CW, LeBreton M, Billong S, Saylors K, Tamoufe U, Papworth E, et al. Influence of stigma and homophobia on mental health and on the uptake of HIV/sexually transmissible infection services for Cameroonian men who have sex with men. Sex Health. 2015;12(4):315–21.
Augustinavicius JL, Baral SD, Murray SM, Jackman K, Xue QL, Sanchez TH, et al. Characterizing cross-culturally relevant metrics of stigma among men who have sex with men across 8 sub-Saharan African Countries and the United States. Am J Epidemiol. 2020;189(7):690–7.
Zlotorzynska M, Sullivan P, Sanchez T. The Annual American men’s internet survey of behaviors of men who have sex with men in the United States: 2015 Key Indicators Report. JMIR Public Health Surveill. 2017;3(1): e13.
Sanchez TH, Sineath RC, Kahle EM, Tregear SJ, Sullivan PS. The Annual American Men’s Internet Survey of behaviors of men who have sex with men in the United States: protocol and key indicators report 2013. JMIR Public Health Surveill. 2015;1(1): e3.
Kaiser H. An index of factorial simplicity. Psychometrika. 1974;39:31–6.
Cerny BA, Kaiser HF. A study of a measure of sampling adequacy for factor-analytic correlation matrices. Multivariate Behav Res. 1977;12(1):43–7.
Muthen B, Muthen L. Mplus User's Guide (8th ed.). 1998–2018;8.
Sass DA, Schmitt TA. A comparative investigation of rotation criteria within exploratory factor analysis. Multivariate Behav Res. 2010;45(1):73–103.
Schmitt TA, Sass DA. Rotation criteria and hypothesis testing for exploratory factor analysis: implications for factor pattern loadings and interfactor correlations. Educ Psychol Meas. 2011;71(1):95–113.
Matsunaga M. How to factor-analyze your data right: do’s, don’ts, and how-to’s. Int J Psychol Res. 2010;3(1):97–110.
Zou G. A modified Poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159(7):702–6.
Aiken LS, West SG. Multiple regression: testing and interpreting interactions. Thousand Oaks: Sage Publications; 1991.
StatCorp LLC. Stata statistical software, release 15. 2017.
Bauer GR, Hammond R. Toward a broader conceptualization of trans women’s sexual health. Can J Hum Sex. 2015;24(1):1–11.
Nemoto T, Bodeker B, Iwamoto M. Social support, exposure to violence and transphobia, and correlates of depression among male-to-female transgender women with a history of sex work. Am J Public Health. 2011;101(10):1980–8.
Reback CJ, Clark K, Holloway IW, Fletcher JB. Health disparities, risk behaviors and healthcare utilization among transgender women in Los Angeles County: a comparison from 1998–1999 to 2015–2016. AIDS Behav. 2018;22(8):2524–33.
Wilson G. Does god bless your transsexual heart: anti-transgender bathroom bills as a newer form of state sanctioned violence note. How Hum Civ Rts L Rev. 2019;3(1):105–28.
Yavorsky JE, Sayer L. “Doing fear”: the influence of hetero-femininity on (trans)women’s fears of victimization. Sociol Quar. 2013;54(4):511–33.
Brumbaugh-Johnson SM, Hull KE. Coming out as transgender: navigating the social implications of a transgender identity. J Homosex. 2019;66(8):1148–77.
Colliver B, Duffus M. Queer space: toilet provision, access and inclusion in the west midlands. Sex Res Soc Policy. 2021;25:1–13.
Seelman KL, Colón-Diaz MJP, LeCroix RH, Xavier-Brier M, Kattari L. Transgender noninclusive healthcare and delaying care because of fear: connections to general health and mental health among transgender adults. Transgend Health. 2017;2(1):17–28.
Tabachnick B, Fidell L, editors. Using multivariate statistics. 6th ed. Boston: Pearson Education, Inc.; 2013.
Maragh-Bass AC, Torain M, Adler R, Ranjit A, Schneider E, Shields RY, et al. Is it okay to ask: transgender patient perspectives on sexual orientation and gender identity collection in healthcare. Acad Emerg Med. 2017;24(6):655–67.
Reisner SL, Perkovich B, Mimiaga MJ. A mixed methods study of the sexual health needs of New England transmen who have sex with nontransgender men. AIDS Patient Care STDS. 2010;24(8):501–13.
Gamarel KE, Nelson KM, Stephenson R, Santiago Rivera OJ, Chiaramonte D, Miller RL, et al. Anticipated HIV stigma and delays in regular HIV testing behaviors among sexually-active young gay, bisexual, and other men who have sex with men and transgender women. AIDS Behav. 2018;22(2):522–30.
Poteat T, Wirtz AL, Radix A, Borquez A, Silva-Santisteban A, Deutsch MB, et al. HIV risk and preventive interventions in transgender women sex workers. Lancet. 2015;385(9964):274–86.
McBride KR, Fortenberry JD. Heterosexual anal sexuality and anal sex behaviors: a review. J Sex Res. 2010;47(2):123–36.
Kutner BA, Simoni JM, King KM, Goodreau SM, Norcini Pala A, Creegan E, et al. Does stigma toward anal sexuality impede HIV prevention among men who have sex with men in the United States? A structural equation modeling assessment. J Sex Med. 2020;17(3):477–90.
Kutner BA, Simoni JM, Aunon FM, Creegan E, Balán IC. How stigma toward anal sexuality promotes concealment and impedes health-seeking behavior in the U.S. among cisgender men who have sex with men. Arch Sex Behav 2020
Diaz RM, Ayala G, Bein E. Sexual risk as an outcome of social oppression: data from a probability sample of Latino gay men in three US cities. Cultur Divers Ethnic Minor Psychol. 2004;10(3):255–67.
Nuttbrock LA, Hwahng SJ. Ethnicity, sex work, and incident HIV/STI among transgender women in New York City: a three year prospective study. AIDS Behav. 2017;21(12):3328–35.
Qiao S, Zhou G, Li X. Disclosure of same-sex behaviors to health-care providers and uptake of HIV testing for men who have sex with men: a systematic review. Am J Mens Health. 2018;12(5):1197–214.
Maksut JL, Eaton LA, Siembida EJ, Fabius CD, Bradley AM. Health care discrimination, sex behavior disclosure, and awareness of pre-exposure prophylaxis among black men who have sex with men. Stigma Health. 2018;3(4):330–7.
Calabrese SK, Underhill K. How stigma surrounding the use of HIV preexposure prophylaxis undermines prevention and pleasure: a call to destigmatize “truvada whores.” Am J Public Health. 2015;105(10):1960–4.
McKirnan DJ, Ostrow DG, Hope B. Sex, drugs and escape: a psychological model of HIV-risk sexual behaviours. AIDS Care. 1996;8(6):655–69.
Alvy LM, McKirnan D, Du Bois SN, Jones K, Ritchie N, Fingerhut D. Health care disparities and behavioral health among men who have sex with men. J Gay Lesbian Soc Serv. 2011;23(4):507–22.
Martin JI, Pryce JG, Leeper JD. Avoidance coping and HIV risk behavior among gay men. Health Soc Work. 2005;30(3):193–201.
Budge SL, Adelson JL, Howard KAS. Anxiety and depression in transgender individuals: the roles of transition status, loss, social support, and coping. J Consult Clin Psychol. 2013;81(3):545–57.
Cahill S. “The Best of Times… the Worst of Times”: what bostock v. clayton county, georgia and the repeal of federal nondiscrimination rules mean for LGBT health. LGBT Health. 2020;7(7):345–8.
Valenti A. LGBT Employment Rights in an evolving legal landscape: the impact of the supreme court’s decision in Bostock v. Clayton County, Georgia. Employee Responsibilities and Rights Journal 2020
Paceley MS, Dikitsas ZA, Greenwood E, McInroy LB, Fish JN, Williams N, et al. The perceived health implications of policies and rhetoric targeting transgender and gender diverse youth: a community-based qualitative study. Transgender Health 2021
Wesp LM, Malcoe LH, Elliott A, Poteat T. Intersectionality research for transgender health justice: A theory-driven conceptual framework for structural analysis of transgender health inequities. Transgend Health. 2019;4(1):287–96.
Acknowledgements
This study was funded by the National Institute of Mental Health (Grant No. R01MH110358) and by the National Institute of Allergy and Infectious Diseases (Grant No. P30AI050409)—the Emory Center for AIDS Research. JLM received research support from the National Institute of Allergy and Infectious Diseases (Grant No. T32AI102623).
Funding
Funding was provided by National Institute of Mental Health (Grant No. R01MH110358), National Institute of Allergy and Infectious Diseases (Grant No. P30AI050409).
Author information
Authors and Affiliations
Contributions
JMW: conceptualization, formal analysis, methodology, visualization, writing (original draft), writing (review & editing); JLM: conceptualization, supervision, writing (review & editing); AIS: writing (review & editing); MZ: writing (review & editing), project administration, data curation; THS: writing (review & editing), project administration, original funding acquisition, original investigation; SDB: writing (review & editing), supervision, project administration, funding acquisition.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to report.
Ethical Approval
The original study was approved by Emory University’s institutional review board. This secondary analysis of de-identified data was deemed exempt from review by Johns Hopkins University’s institutional review board.
Consent to Participate
This was a secondary data analysis of de-identified data. In the original study, participants provided informed consent to participate.
Consent for Publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wiginton, J.M., Maksut, J.L., Scheim, A.I. et al. Intersecting Sexual Behavior and Gender Identity Stigmas Among Transgender Women in the United States: Burden and Associations with Sexual Health. AIDS Behav 27, 3064–3079 (2023). https://doi.org/10.1007/s10461-023-04028-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-023-04028-w