
Abstract
Aim
To evaluate two microbiological diagnostic methods with sputum samples for pulmonary tuberculosis, for quantifying the inherent errors in each method, based on Bayes rule.
Subject and methods
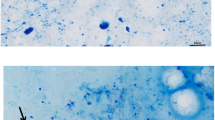
Diagnostic test results of 1,064 sputum samples were obtained by smear microscopy (Ziehl-Neelsen staining) or the smear test and with the other popular and assertive method, the culturing of samples on the Lowenstein-Jensen medium or the culture test. Results were subjected to a Bayesian analysis.
Results
In the diagnostic analysis of 1,064 samples, there were 143 true-positives, 05 false-positives, 675 true-negatives and 241 false-negatives. Probability values of the analysis are given. The prevalence or a priori probability (the pre-test prevalence of disease in the targeted population) value = 0.3609; the sensitivity (true positive rate or probability of smear test positives among culture positives) was 0.3724, whereas the specificity (true negative rate or probability of smear test negatives among culture test negatives) was 0.9926. The false positive rate (probability of errors of the culture test) = 0.00735; the false negative rate (probability of errors of the smear test) = 0.6276; the positive predictivity (post-test probability of the disease that gave a positive result) and the negative predictivity (post-test probability of the disease that gave a negative result) values were 0.9662 and 0.7369, respectively. Computed values of other test statistics were: diagnostic accuracy (accuracy of diagnosing positivity/negativity of tests) = 0.7688; positive likelihood ratio (ratio of true positive rate and false positive rate) = 50.66; negative likelihood ratio (ratio of false negative rate and true negative rate) = 0.6322; and a posteriori probability (post-test arithmetic computation for diagnostic efficiency) = 0.5738. The area under the receiver operating characteristic (ROC curve or the AUC (post-test graphical analysis for diagnostic efficiency) was 0.648.
Conclusion
The prevalence of the disease was 36 %. The smear test was efficient by 37–97 % in arriving at a positive result with a sample, when its culture test was positive; alternately, it was efficient by 74–99 % for a negative result, when its culture test result was negative. As found by post-test analysis, both smear and culture tests were dependable by 57–65 % for pulmonary tuberculosis.


Similar content being viewed by others

References
Akmatov MK, Mikolajczyk RT, Krumkamp R, Wörmann T, JunQing Chu J, Paetzelt G, Reintjes R, Pessler F, Krämer A (2012) Availability of indicators of migration in the surveillance of HIV, tuberculosis and hepatitis B in the European Union : a short note. J Publ Health doi: 10.1007/s10389-011-0488-1
Altman DG, Bland JM (1994) Statistics notes: diagnostic tests 2: predictive values. British Med J 309:102–109
Boehme CC, Nabeta P, Hilleman D, Nicol MP, Shenai S, Krapp F et al (2010) Rapid molecular detection of tuberculosis and rifampicin resistance. N Engl J Med 363:1005–1015
Dubey D, Rath S, Sahu MC, Nayak N, Debata NK, Padhy RN (2012) Status of multidrug resistance in tubercle bacillus and phytochemicals for the control. J Publ Health doi:10.1007/s10389-012-0514-y
Frieden T (ed) (2004) Toman’s tuberculosis: case detection, treatment and monitoring: questions and answers, 2nd edn. Available at http://www.who.int/tb/publications/toman/en/index.html. Accessed 26 April 2012
Idrees M, Bhatti AH, Khan SU, Riazuddin S (1998) Drug resistance in M. tuberculosis isolated from a group of patients referred to PMRC, TB Research Center at Mayo Hospital, Lahore, Pakistan. Pakistan J Zool 30:335–339
Iqbal S, Idrees M, Shabbir I, Khan MM, Riazuddin S (2001) TB case management by doctors. Pakistan J Med Res 40:64–68
Janssens J-P, Roux-Lombard P, Perneger T, Metzger M, Vivien R (2007) Rochat T (2007) Quantitative scoring of an interferon-γ assay for differentiating active from latent tuberculosis. Eur Respir J 30:722–727. doi:10.1183/09031936.00028507
Kaminski DA, Hardy DJ (1995) Selective utilization of DNA probes for identification of Mycobacterium species on the basis of cord formation in primary BACTEC 12B cultures. J Clin Microbiol 33:1548–1550
Mahon CR, Mahon C, Lehman DC, Manuselis G, Manuselis G Jr (2010) Text book of diagnostic microbiology. Saunders, Philadelphia, PA, pp 636–676
Rodrigues C (2011) Diagnostics for tuberculosis: time to user in the new era. Indian J Med Microbiol 29:2–3
Rosner B (2000) Fundamentals of biostatistics, 5th edn. Duxbury, Pacific Grove, CA
Schaberg T, Rebhan K, Lode H (1996) Risk factors for side-effects of isoniazid, rifampin and pyrazinamide in patients hospitalized for pulmonary tuberculosis. Eur Respir J 9:2026–2030
Singh S (2008) Scaling up anti-mycobacterial drug susceptibility testing services in India: it is high time. Indian J Med Microbiol 26:209–211
Takahashi S (1975) Handbook of direct smear examinations of sputum for tubercle bacilli. The South-East Asian Medical Information Centre, Tokyo
WHO (2011) WHO report 2011: Global tuberculosis control.. Available at: http://www.who/htm/tb/2011.16. Accessed 20 December 2011
Yeager H Jr, Lacy J, Smith LR, LeMaistre CA (1967) Quantitative studies of mycobacterial populations in sputum and saliva. Am Rev Respir Dis 95:998–1004
Zhou XH, Obuchowski NA, McClish DK (2011) Statistical methods in diagnostic medicine, 2nd edn. Wiley, New York. doi:10.1002/9780470906514
Ziaee M, Namaei M, Khazaei M, Azarkar G (2008) Comparison of the values of two different sputum staining methods for diagnosis of acid-fast bacilli. Iran J Clin Infect Dis 3:99–102
Acknowledgements
This work is a part of PhD thesis MC Sahu in Biotechnology of Utkal University and he is a Project Fellow in a Major Research Project in Botany, ‘Alternative drug search from ethnomedicinal plants of Odisha against multidrug resistant bacteria’, grant no. 39-388/2010/SR, supported by University Grants Commission, New Delhi, awarded to RN Padhy. We are grateful to Prof. Dr. DK Roy, Dean, IMS and Sum Hospital for facilities and Dr. Susama Tripathy, Principal, BJB Autonomous College for encouragements, and to Prof. Dr. RP Mohanty, the Honourable Vice Chancellor, S‘O’A University for an interest in the work.
Conflict of interest
The authors confirm that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sahu, M.C., Rath, S., Dubey, D. et al. Evaluation of two microbiological diagnostic methods for pulmonary tuberculosis based on Bayes rule. J Public Health 21, 123–130 (2013). https://doi.org/10.1007/s10389-012-0517-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-012-0517-8