
Abstract
Degenerative changes in the lumbar spine can be followed by cystic changes. Most reported intraspinal cysts are ganglion or synovial cysts. Ligamentum flavum pseudocyst, as a cystic lesion in the lumbar spine, is a rare and unusual cause of neurologic signs and symptoms and is usually seen in elderly persons (due to degenerative changes). They are preferentially located in the lower lumbar region, while cervical localization is rare. Complete removal of the cyst leads to excellent results and seems to preclude recurrence. We report the case of a right-sided ligamentum flavum cyst occurring at L3–L4 level in a 70-year-old woman, which was surgically removed with excellent postoperative results and complete resolution of symptoms. In addition, we discuss and review reports in the literature.
Similar content being viewed by others


Introduction
Different etiologies for cystic lesions in the lumbar spinal canal have been reported in the literature, among them hemorrhagic cysts, perineural cysts, dermoid cysts, and parasitic cysts [4]. The most common lesion seems to originate from the facet joints: the synovial cyst, which represents a protrusion of the synovial membrane into the surrounding tissue. The literature remains imprecise about the histopathologic nature of cystic lesions in the lumbar region of the spine. Some authors differentiate between the terms “synovial cyst” (with a synovial lining) and “ganglion pseudocyst” (without any synovial lining). Others proposed the term “juxtafacet cyst,” simply representing both. Also, evolution from a synovial cyst into a ganglion pseudocyst has been questioned. Ligamentum flavum pseudocyst, as a cystic lesion in the lumbar spine, has only rarely been mentioned [4, 5, 7, 25, 28, 29].
Case report
A 70-year-old woman presented with 5-year history of gradually developing gait disturbance as well as pain in the lumbar area, buttock, and right leg, particularly the right knee, involving mostly the L4 distribution. In the meantime an artificial knee joint was implanted with inadequate recovery of the pain. The pain did not improve substantially with conservative therapy. On clinical examination, motor function was normal and there was no sensory disturbance on examination of the legs. Reflexes were hypoactive in both legs with right-sided patellar reflex loss. Magnetic resonance imaging revealed at L3–L4 level a right-sided voluminous epidural cystic lesion, 10 mm in diameter, which was hypointense on T1-weighted images and hyperintense on T2-weighted images and its wall was enhanced with contrast material. The mass displaced the dural sac anteriorly and resulted in marked stenosis of the spinal canal. The mass was surgically resected together with the hypertrophied ligamentum flavum after partial L3–L4 hemilaminectomy (Fig. 1). A round, yellowish cyst of about 10 mm in diameter filled with somewhat gelatinous fluid and barely adhered to the dura mater was found. There was no connection between the cyst and the facet joint. Pathological examination of the cyst revealed myxoid and pseudocystic degeneration of the ligamentum flavum (Fig. 2). There was no synovial lining. The patient’s postoperative course was uneventful, with complete resolution of symptoms. After 10 months follow-up the patient continues to do very well. She is neurologically intact and symptom free. The patient provided her consent to the publication of this case report.

Intraoperative view via the surgical microscope showing part of the cyst and degenerated ligamentum flavum (arrow), regular ligamentum flavum (notched arrow), and dura mater spinalis (arrowhead)

Histopathologic section of operative specimen reveals degenerative changes in the ligamentum flavum with infiltration of inflammatory cells and no synovial cell lining (hematoxylin and eosin)
Discussion
Several studies have shown that the usual aging process of the ligamentum flavum causes thickening and loss of elasticity [11]. Change in proteoglycans, loss of elastic fibers, and increase in collagen tissue and chondroid metaplasia due to mechanical stress have been described [22]. Additionally and closely related to age, amyloid can accumulate within the ligamentum flavum [25]. This amyloid deposition has been reported in only a few cases to be associated with systemic amyloidosis [24]. Similarly, age-related calcification of the ligamentum flavum can occur [26]. A diffuse form of calcification contributing to the loss of elasticity and the thickening and a focal form of calcified material accumulation as well as granulomatous inflammation and tophaceous depositions of calcium pyrophosphate crystals can occur. These depositions have been ascribed to decreasing cellularity of the ligamentum flavum with age and resultant diminished calcification inhibiting factor production by fibroblastic-like cells [21]. The tophaceous type of lesion seems to be closely related to previous degeneration of the affected ligament by minor trauma predisposing to calcium deposition. Activity of proteolytic enzymes within the ligament, produced by neutrophils localizing to calcified nodules, has been found [9]. Wildi et al. [30] found only four patients with calcium pyrophosphate depositions, suggesting that they play a minor role in the pathogenesis of ligamentum flavum pseudocysts. In addition to calcification, ossification of the ligamentum flavum might occur. This seems to follow a sequential process of chondroid metaplasia and eventual enchondral ossification mainly at the insertion site of the ligament. All these factors, resulting partially from mechanical stress, seem to contribute to loss of the natural structure of the ligamentum flavum, making them again susceptible to new mechanical stress, forming a vicious circle. The degenerated bony structure of the lumbar spine and the facet joints suggest a major pathogenic role of degenerative segmental instability in pseudocyst formation of the ligamentum flavum, as found by other authors too [18]. Most ligamentum flavum cysts reported in the literature were also located laterally within the spinal canal. While possibly a consequence of chronic bony degenerative disease, this phenomenon may be further elucidated in certain cases by the observation that the yellow ligaments are not as thick laterally as they are medially. Furthermore, they form posterior recesses bilaterally to the vertebral bodies. These recesses are filled with epidural fat [16] and offer an area of decreased resistance and may, as a result, tolerate cyst formation.
The pathogenesis of ligamentous degeneration remains to be elucidated, but it may be considered in the context of degenerative spinal changes. The spine is divided into alternating mobile and fixed segments, and the transitional zones between the mobile and fixed regions incur the most severe stress during motion. The anatomic disposition, histologic characteristics, and biomechanical properties of the ligamentum flavum indicate that it is markedly different from other spinal ligaments [10]. The ligamentum flavum is a well-defined elastic structure composed of 80% elastic and 20% collagen fibers [31]. This composition of dense connective tissue with elastic fiber predominance is rarely seen in other tissues, although it can be seen in the vestibular folds of the larynx and the media of large arteries [31]. When a change occurs in the ligamentum flavum, regeneration of elastic fibers that includes the formation of collagen fibers and degenerative changes occurs, and this regenerative process leads to decrease in elasticity. Moreover, this process in the ligamentum flavum is markedly different from other spinal ligamentous reactions [10]. Thus, chronic irritative or degenerative changes of the ligamentum flavum in the area of the cyst could predispose it to mechanical stress, even after a minor repeated injury [8].
Cysts of the ligamentum flavum have myxoid degeneration and arise from or are partially embedded in the inner surface of this ligament, and in contrast to juxta-articular cysts, are not related to the facet joint cavity. Pathogenesis of the cyst formation is secondary to ligamentous and fibrocollagenous tissue degeneration and hypermobility of the spinal segment, mainly at the transitional zones between the mobile and the fixed segments of the spine [14]. These degenerative changes represent a histologically distinct entity different from ganglion or synovial cysts. Pathologic ligamentum flavum cysts can contain hemorrhage, and previous degeneration of the ligament may create conditions for the formation of hematoma. Rupture of vessels in degenerated lumbar ligamentum flavum may develop secondary to stretching forces on the back. The pathogenesis of the hematoma may originate from minor acute or chronic trauma such as minor back injury, physical exertion or heavy lifting [20, 26].
Intraspinal ligamentum flavum cysts are rare; they occur preferentially in the lower lumbar region [5, 15, 32], while cervical localization is uncommon [17]. In most of the cases, ligamentum flavum cysts in the lumbar spine occur at L4–L5, the most mobile segment within the lumbar spine, and are frequently associated with lumbar degenerative spondylolisthesis. Cervical cysts are preferentially located in the cervicothoracic junction [29]. Continuous stress to the ligamentum flavum due to minor chronic trauma such as listhesis may predispose to the formation of the cyst [8]. Only in a few cases is the localization of cysts C6–C7, C3–C4, and C5–C6 levels [29]. No reports have described the appearance of these cysts in any region other than the mobile spine. The T2–10 vertebrae mainly act with the ribs to form the thorax and are not generally considered to be part of the mobile spine (Table 1).
There are no specific clinical symptoms for ligamentum flavum cyst. Cysts in the spinal canal can impinge upon and displace neural structures and can lead to neurologic symptoms. The majority of symptomatic cysts usually presents with radiculopathy, such as sciatica in the case of lumbar cysts, and can mimic symptoms related to intervertebral disc herniation [15]. In the study of Wildi et al. [30], 97% patients complained of radicular pain, 39% showed motor deficits, 55% had sensory changes, 18% had abnormal reflexes, and 33% showed a positive Lasèque sign. Our patient presented with gradually developing right-sided radicular pain involving mostly the L4 distribution with patellar reflex loss on the same side.
Neuroimaging is helpful in diagnosing cyst of the ligamentum flavum. On myelography, these lesions are recognized as intraspinal extradural masses and on postmyelogram computed tomography as a faint cyst adjacent to the ligamentum flavum [32]. Magnetic resonance imaging provides the best images [14, 20, 25, 28]: on T1-weighted images, the cysts have a variable signal, and on T2-weighted images, the cysts have a high-intensity signal [20, 28]. Differential diagnosis of imaging studies between ligamentum flavum cysts and synovial cysts is useful to the surgeon, as the latter are more difficult to resect, requiring exploration of the facet joint. Magnetic resonance imaging, in some cases of synovial cysts, reveals demonstrable communication with the facet joint with enhancement of the synovial cyst wall and of the adjacent facet joint. Synovial cysts often have a calcified rim, while ligamentum flavum cysts do not. In our study, magnetic resonance imaging revealed at L3–L4 level a right-sided voluminous epidural cystic lesion, 10 mm in diameter, which was hypointense on T1-weighted images (Fig. 3a, b) and hyperintense on T2-weighted images (Fig. 4) and its wall was enhanced with contrast material (Fig. 3c, d). The computed tomography appearance of synovial cysts is often diagnostic and correlates well with pathologic findings. They typically consist of a cystic formation whose walls show calcification, and are located adjacent to facet joints that frequently show signs of degeneration [9]. Ligamentum flavum cysts, conversely, have not been observed to cause rim calcification. Juxtafacet cysts appear as well-delineated cystic masses; the rim of synovial cysts is typically isointense to slightly hyperintense compared with cerebrospinal fluid in T1 and hypointense in T2, and its contents have variable intensities and several classifications have been proposed. In the case of ligamentum flavum cysts, they are seen adjacent to the ligamentum flavum [23] and there is no observable communication with the spinal facet joint. When intraluminal hemorrhage occurs in a minority of cases, they are easier to distinguish from herniated disk fragments and most neoplasms [20]. In addition to other cystic lesions that may affect the lumbar spine, calcium pyrophosphate dihydrate deposits have been observed in the ligamentum flavum among patients presenting with lumbar pain and/or radiculopathy, and typically are hypointense on magnetic resonance imaging and show calcifications on computed tomography imaging.

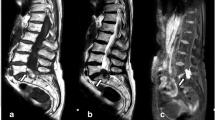
T1-weighted magnetic resonance image demonstrating a hypointense intraspinal extradural right-sided ligamentum flavum cyst (white arrow): a sagittal pre-gadolinium, b axial pre-gadolinium, c sagittal post-gadolinium, d axial post-gadolinium

T2-weighted magnetic resonance image showing a hyperintense signal of the above-mentioned cyst (white arrow): a sagittal, b axial
Differential diagnosis of intraspinal extradural mass lesions includes ligamentum flavum cyst, juxta-articular cysts (ganglion and synovial cysts), arachnoid cyst, perineural cyst, dermoid cyst, infectious cyst, schwannoma, meningioma, and metastasis or nontumorous-type mass lesions including neurofibromas, fibrous dysplasia, ependymal cyst, and rheumatoid arthritis pannus [15, 20, 23]. The nomenclature of cysts in the spinal canal is somewhat unclear in the literature. Most intraspinal cysts reported are juxta-articular cysts. Ligamentum flavum and juxta-articular cysts can be definitely distinguished only by their pathological findings.
Conservative therapy appears to have no success [15, 20]. Most conservative therapies are temporary and have varying success in the short term. Surgical removal is the first-choice therapy. The goal of surgery is spinal decompression as well as resection of the cyst and affected ligamentum flavum. Complete excision at the base of the ligamentous insertion of the cyst assures a minimal rate of recurrence. Wildi et al. [30] reported recurrence of the cyst in the remaining ligamentum flavum in two patients 1 year after surgery. While nearly 95% of all operated cysts can be removed in their entirety, a major reported intraoperative difficulty lies in the presence of adhesions to the dural wall, which is the main causative factor of incomplete resection [9].
Complete removal of pseudocystic lesions generally has excellent results [2, 9, 14, 27, 28, 30]. Our patient showed complete postoperative resolution of symptoms. She is neurologically intact and symptom free to date.
To summarize, ligamentum flavum cysts represent a rare cause of lumbar nerve root compression or spinal stenosis. The lumbar ligamentum flavum undergoes lifelong mechanical stress. Similar to bony structures in this region, it degenerates with age. The degenerative changes in the lumbar ligamenta flava can be followed by cystic changes. Histologically, these degenerative changes represent a distinct entity different from ganglion or synovial cysts. Magnetic resonance imaging provides the best images. Radical removal of pseudocyst guarantees in nearly all cases complete relief of radiculopathy and seems to prevent recurrence of such a lesion at the same level.
References
Abdullah AF, Chambers RW, Daut DP (1984) Lumbar nerve root compression by synovial cysts of the ligamentum flavum. Report of four cases. J Neurosurg 60(3):617–620
Asamoto S, Jimbo H, Funkui Y, Doi H, Sakgawa H, Ida M, Takahashi M, Shiraishi N (2005) Cyst of the ligamentum flavum—case report. Neurol Med Chir (Tokyo) 45(12):653–656
Ayberk G, Ozveren F, Gök B, Yazgan A, Tosun H, Seçkin Z, Altundal N (2008) Lumbar synovial cysts: experience with nine cases. Neurol Med Chir (Tokyo) 48(7):298–303; discussion 303
Baker JK, Hanson GW (1994) Cyst of the ligamentum flavum. Spine 19:1092–1094
Barlocher CB, Seiler RW (2000) Vertebral erosion and a ligamentum flavum cyst. Case illustration. J Neurosurg 93(2 Suppl):335
Bloch J, Hawelski S, Benini A (1997) Cyst of the ligamentum flavum of the lumbar spine: description of 6 cases. Schweiz Med Wochenschr 26;127(17):728–732
Cakir E, Kuzeyli K, Usul H, Peksoyulu B, Yazar U, Reis A, Karaarslan G (2004) Ligamentum flavum cyst. J Clin Neurosci 11:67–69
Chan LF, Lui CC, Cheng MH, Lin WJ (1996) Ganglion cyst in the ligamentum flavum of the cervico-thoracic junction. J Formos Med Assoc 95:490–492
DiMario S, Marmor E, Albrecht S, Mohr G (2005) Ligamentum flavum cysts causing incapacitating lumbar spinal stenosis. Can J Neurol Sci 32:237–242
Fuertes DV, Liguoro D, Rivel J (1998) Morphologic and histologic study of the ligamentum flavum in the thoraco-lumbar region. Surg Radiol Anat 20:171–176
Fukuyama S, Nakamura T, Ikeda T et al (1995) The effect of mechanical stress on hypertrophy of the lumbar ligamentum flavum. J Spinal Disord 8:126–130
Furusawa N, Baba H, Maezawa Y et al (1997) Calcium crystal deposition in the ligamentum flavum of the lumbar spine. Clin Exp Rheumatol 15:641–647
Gazzeri R, Canova A, Fiore C, Galarza M, Neroni M, Giordano M (2007) Acute hemorrhagic cyst of the ligamentum flavum. J Spinal Disord Tech 20(7):536–538
Gazzeri R, Galarza M, Gorgoglione L, Bisceglia M, D’Angelo V (2005) Cervical cyst of the ligamentum flavum and C7-T1 subluxation: case report. Eur Spine J 14:807–809
Haase J (1972) Extradural cyst of the ligamentum flavum L4: a case. Acta Orthop Scand 43:32–38
Harrison GR (1999) Topographical anatomy of the lumbar epidural region: an in vivo study using computerized axial tomography. Br J Anaesth 83:229–234
Hatem O, Bedou G, Negre C, Bertrand JL, Camo J (2001) Intraspinal degenerative cyst. J Neurosurg (Spine) 95:139–142
Howington JU, Connolly ES, Voorhies RM (1999) Intraspinal synovial cysts: 10-year experience at the Ochsner clinic. J Neurosurg (Spine 2) 91:193–199
Lunardi P, Acqui M, Ricci G, Agrillo A, Ferrante L (1999) Cervical synovial cysts: case report and review of the literature. Eur Spine J 8(3):232–237
Mahallati H, Wallace K, Hunter M, Bilbao J, Clark A (1999) MR imaging of a hemorrhagic and granulomatous cyst of the ligamentum flavum with pathologic correlation. AJNR 20:1166–1168
Maruta K, Ichimura K, Matsui H et al (1993) Calcification inhibitors in human ligamentum flavum. J Orthop Res 11:92–103
Okada A, Harata S, Takeda Y et al (1993) Age-related change in proteoglycans of human ligamentum flavum. Spine 18:2261–2266
Olivier V, Heinz F, Pierre S, Jean Pierre D (1991) Cyst of the ligamentum flavum: report of six cases. Neurosurgery 29:277–283
Roche PH, Figarella-Branger D, Malca S et al (1999) Lumbar canal stenosis caused by amyloidosis of the yellow ligament. Neurochirurgi 45:91–97
Savitz MH, Sachdev VP (1992) Cyst of the ligamentum flavum: report of six cases. Neurosurgery 30:461–462
Schrader PK, Grob D, Rahn BA et al (1999) Histology of the ligamentum flavum in patients with degenerative lumbar spinal stenosis. Eur Spine J 8:323–328
Takano Y, Homma T, Okumura H, Takahashi HE (1992) Ganglion cyst occurring in the ligamentum flavum of the cervical spine. A case report. Spine 17:1532–1533
Terada H, Yokoyama Y, Kamata N, Hozumi T, Kondo T (2001) Cyst of the ligamentum flavum. Neuroradiology 43:49–51
Vernet O, Frankhauser H, Schnyder P et al (1991) Cyst of the ligamentum flavum: report of six cases. Neurosurgery 29:277–283
Wildi LM, Kurrer MO, Benini A, Weishaupt D, Michel BA, Brühlmann P (2004) Pseudocystic degeneration of the lumbar ligamentum flavum. A little known entity. J Spinal Disord Tech 17:395–400
Yahia LH, Newman N, Rivard CH (1990) Light and scanning electron microscopy of human spinal ligamentum flavum. A preliminary study. Spine 15:262–268
Yamamoto A, Nishiura I, Handa H et al (2001) Ganglion cyst in the ligamentum flavum of the cervical spine causing myelopathy: report of two cases. Surg Neurol 56:390–395
Conflict of interest
None.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Taha, H., Bareksei, Y., Albanna, W. et al. Ligamentum flavum cyst in the lumbar spine: a case report and review of the literature. J Orthopaed Traumatol 11, 117–122 (2010). https://doi.org/10.1007/s10195-010-0094-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10195-010-0094-y