
Abstract
Background
We investigated factors associated with the anti-severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike antibody titer after the second dose of the BNT162b2 messenger RNA coronavirus disease 2019 (COVID-19) vaccine in Japanese patients undergoing hemodialysis.
Methods
Overall, 75 patients (41 men, 34 women; mean age 71.4 ± 12.2 years) with a hemodialysis duration of 5.7 ± 6.1 [interquartile range, 1.0–8.5] years were enrolled in this single-center, prospective, cross-sectional study. We used multiple linear regression analysis to determine the relationships of the anti-SARS-CoV-2 spike antibody titer with patient demographic and clinical parameters. We also compared the anti-SARS-CoV-2 spike antibody titer between hemodialysis patients and 22 healthcare workers (10 men, 12 women; mean age 48.5 ± 14.4 years).
Results
Autoimmune disease presence (standard coefficient [β] = − 0.290, p = 0.018), lymphocyte counts (β = 0.261, p = 0.015), hemoglobin levels (β = 0.290, p = 0.009), and blood urea nitrogen concentrations (β = 0.254, p = 0.033) were significantly and independently correlated with the log-anti-SARS-CoV-2 spike antibody titer. The anti-SARS-CoV-2 spike antibody titer was significantly lower in hemodialysis patients than in healthcare workers (3589 ± 3921 [813–4468] vs. 12,634 ± 18,804 [3472–10,257] AU/mL; p < 0.002).
Conclusions
Autoimmune disease presence, lymphocyte counts, hemoglobin levels, and blood urea nitrogen concentrations were associated with the anti-SARS-CoV-2 spike antibody titer after the second dose of the BNT162b2 messenger RNA COVID-19 vaccine in Japanese patients undergoing hemodialysis.
Similar content being viewed by others


Introduction
The coronavirus disease 2019 (COVID-19) vaccine is critical for preventing COVID-19 infection and controlling the ongoing global pandemic. One study reported that the anti-severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike antibody titer was related to the risk of COVID-19 infection after COVID-19 vaccination [1]. Therefore, determining a sufficient anti-SARS-CoV-2 spike antibody titer is important to help prevent breakthrough COVID-19 infections.
Various factors, such as age, sex, alcohol consumption, and immunosuppressant use, have been reported to be associated with the anti-SARS-CoV-2 spike antibody response after COVID-19 vaccination in healthcare workers [2, 3]. Recent studies also revealed that age, immunosuppressive treatments, and lymphocyte counts were associated with the anti-SARS-CoV-2 spike antibody response after COVID-19 vaccination in individuals undergoing hemodialysis [4,5,6]. However, factors related to the anti-SARS-CoV-2 spike antibody response after COVID-19 vaccination have not been determined in Asian individuals undergoing hemodialysis. We conducted the present study to investigate the various demographic and clinical factors associated with the anti-SARS-CoV-2 spike antibody titer after the second dose of the COVID-19 vaccine in Japanese patients undergoing hemodialysis.
Patients and methods
Ethical approval
This study was approved by the Ethical Committee of Mizue Yuai Clinic (MYC 2021-01) and carried out in accordance with the fundamental principles within the Declaration of Helsinki. Written informed consent was obtained from all participants.
Patients
The inclusion criteria for patients were as follows: (i) aged ≥ 20 years, (ii) chronic kidney disease stage G5D, (iii) currently undergoing hemodialysis, and (iv) vaccinated with two doses of the BNT162b2 messenger RNA (mRNA) COVID-19 vaccine (Pfizer Inc., and BioNTech) with the recommended dosing interval of 3 weeks between the first and second doses. The exclusion criteria were as follows: (i) unwilling or unable to give consent and (ii) any history of COVID-19 infection. Healthcare workers who were vaccinated twice with the BNT162b2 mRNA COVID-19 vaccine and gave informed consent to participate were used as the control group.
Study design
This was a single-center, prospective, cross-sectional study conducted between April 1, 2021 and August 31, 2021 at Mizue Yuai Clinic, Tokyo. Each participant’s anti-SARS-CoV-2 spike antibody titer was measured 4 weeks after the second dose of the BNT162b2 mRNA COVID-19 vaccine. Demographic and clinical parameters were collected at the time of anti-SARS-CoV-2 spike antibody titer measurements. Multiple linear regression analysis was conducted to analyze factors independently associated with the anti-SARS-CoV-2 spike antibody titer. We also compared the anti-SARS-CoV-2 spike antibody titers between hemodialysis patients (hemodialysis patient group) and healthcare workers (control group).
Laboratory methods
Hemodialysis patient blood samples were obtained from an arteriovenous fistula just before the initiation of their first hemodialysis session of the week. Blood parameters and anti-SARS-CoV-2 spike antibody titers were measured at a commercial laboratory (BML, Tokyo, Japan). Anti-SARS-CoV-2 spike antibody titers were determined using the SARS-CoV-2 IgG II Quant assay (Abbott, Sligo, Ireland). The normalized protein catabolism rate and single-pool urea clearance were calculated using the formula reported by Shinzato [7].
Statistical analyses
Continuous variables with a normal distribution are expressed as the mean ± standard deviation, and those with a non-normal distribution are reported as the mean ± standard deviation [interquartile range]. Categorical variables are expressed as numbers and percentages. The duration of hemodialysis, level of C-reactive protein, and anti-SARS-CoV-2 spike antibody titer did not show normal distributions, and these variables were transformed using the natural logarithm. A comparison of anti-SARS-CoV-2 spike antibody titers between hemodialysis patients and healthcare workers was performed using the Mann–Whitney U test. Parameters that appeared to be significantly correlated with the anti-SARS-CoV-2 spike antibody titer in simple linear regression analyses (p < 0.10) were included in the multiple linear regression analysis to identify factors correlated with the anti-SARS-CoV-2 spike antibody titer. A p value < 0.05 was considered significant. Statistical analyses were performed using JMP 11 software (SAS, Cary, NC, USA).
Results
Patient characteristics
The demographic and clinical characteristics of the hemodialysis patient and control groups are summarized in Table 1. The hemodialysis patient group included 41 male patients and 34 female patients, with a mean age of 71.4 ± 12.2 years, body mass index of 22.0 ± 4.1 kg/m2, and hemodialysis duration of 5.7 ± 6.1 [1.0–8.5] years. Fourteen patients (18.7%) had a past or current smoking history, and 12 patients (16.0%) had an alcohol consumption habit. The percentages of patients with diabetes mellitus, hypertension, allergic diseases, and autoimmune diseases were 46.7%, 52.0%, 22.7%, and 12.0%, respectively. The proportions of patients with a history of infection were as follows: hepatitis B virus infection, 26.7%; hepatitis C virus infection, 5.3%; and syphilis infection, 8.0%. Among nine patients with autoimmune diseases, three were taking corticosteroids, and six were not taking corticosteroids. The control group consisted of 22 healthcare workers (10 men, 12 women, mean age 48.5 ± 14.4 years, body mass index 23.7 ± 5.4 kg/m2). Ten workers (45.5%) had a past or current smoking history, and 15 workers (68.2%) had an alcohol consumption habit. The percentages of workers with diabetes mellitus, hypertension, allergic diseases, and autoimmune diseases were 9.1%, 27.3%, 40.9%, and 0.0%, respectively. No worker had any history of hepatitis B virus, hepatitis C virus, or syphilis infection.
Medication use among patients was as follows: corticosteroids, 5.3%; renin–angiotensin system inhibitors, 37.3%; statins, 30.7%; erythropoiesis-stimulating agents, 86.7%; hypoxia-inducible factor prolyl hydroxylase inhibitors, 8.0%; iron supplements, 65.3%; zinc supplements, 14.7%; phosphate binders, 80.0%; vitamin D analogs, 81.3%; and calcimimetics, 37.3%. None of the healthcare workers received any medications, except for five workers (renin–angiotensin system inhibitors, n = 2; statins, n = 3).
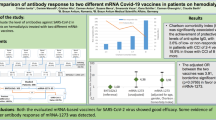
The anti-SARS-CoV-2 spike antibody titer in hemodialysis patients was 3589 ± 3921 [813–4,468] AU/mL. The distribution of patients according to their anti-SARS-CoV-2 spike antibody titers is shown in Fig. 1a. The anti-SARS-CoV-2 spike antibody titer was not significantly different between patients with autoimmune diseases treated with or without corticosteroids (1087 ± 1240 vs. 2347 ± 877; p = 0.37). The distribution of healthcare workers according to their anti-SARS-CoV-2 spike antibody titers is shown in Fig. 1b. Other clinical parameters were not measured among healthcare workers.

a Distribution of hemodialysis patients according to their anti-severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike antibody titers. b Distribution of healthcare workers according to their anti-SARS-CoV-2 spike antibody titers
Factors associated with the log-anti-SARS-CoV-2 spike antibody titer after the second BNT162b2 mRNA COVID-19 vaccination
Simple linear regression analyses showed that the log-anti-SARS-CoV-2 spike antibody titer was significantly correlated with autoimmune disease presence and hemoglobin, sodium, and chloride levels. We performed a multiple linear regression analysis using the variables that showed marginal or significant correlations (p < 0.10) with the log-anti-SARS-CoV-2 spike antibody titer in simple linear regression analyses (Table 2). This analysis revealed that autoimmune disease presence (standard coefficient [β] = − 0.290, p = 0.018), lymphocyte counts (β = 0.261, p = 0.015), hemoglobin (β = 0.290, p = 0.009), and blood urea nitrogen (BUN) (β = 0.254, p = 0.033) were independently correlated with the log-anti-SARS-CoV-2 spike antibody titer.
Comparison of anti-SARS-CoV-2 spike antibody titers between hemodialysis patients and the control group
The anti-SARS-CoV-2 spike antibody titer was significantly lower in hemodialysis patients that in healthcare workers (3589 ± 3921 [813–4468] vs. 12,634 ± 18,804 [3472–10,257], p < 0.002; Fig. 2).

Comparison of the anti-SARS-CoV-2 spike antibody titer between hemodialysis patients (n = 75) and healthcare workers (n = 22) (*p = 0.002)
Discussion
We identified factors associated with the anti-SARS-CoV-2 spike antibody titer after the second dose of the COVID-19 vaccine in Japanese hemodialysis patients. Multiple linear regression analysis revealed that autoimmune disease presence, lymphocyte counts, hemoglobin levels, and BUN concentrations in hemodialysis patients were independently correlated with the anti-SARS-CoV-2 spike antibody titer after the second dose of the COVID-19 vaccine. The anti-SARS-CoV-2 spike antibody titer was significantly lower in hemodialysis patients that in healthcare workers.
Recent studies reported that the lymphocyte count was positively associated with the anti-SARS-CoV-2 spike antibody response in hemodialysis patients who received a COVID-19 vaccination [4,5,6]. Our present findings also revealed that the lymphocyte count was positively and significantly correlated with the anti-SARS-CoV-2 spike antibody titer after COVID-19 vaccination in hemodialysis patients. These results suggest that the lymphocyte count may predict the humoral immune response after COVID-19 vaccination in patients undergoing hemodialysis. Autoimmune diseases were reported to negatively affect antibody production after vaccination [8, 9]. Our present analyses indicated that after adjusting for covariates, including corticosteroid use and lymphocyte counts, autoimmune disease presence was independently and negatively associated with the anti-SARS-CoV-2 spike antibody titer. These results suggest that autoimmune diseases may lead to a weaker humoral immune response to COVID-19 vaccines in hemodialysis patients. Anemia diminishes adaptive immune responses, including cell-mediated and humoral immunity [10]. In the present study, the hemoglobin concentration in hemodialysis patients was positively correlated with the anti-SARS-CoV-2 spike antibody titer after COVID-19 vaccination. These findings suggest that maintaining a higher hemoglobin level might augment the anti-SARS-CoV-2 spike antibody response in hemodialysis patients after they receive a COVID-19 vaccination. Further studies are required to investigate whether maintaining a higher hemoglobin level leads to a greater anti-SARS-CoV-2 spike antibody response in hemodialysis patients after COVID-19 vaccination. BUN, derived from protein catabolism, is a major nutritional parameter in hemodialysis patients [11]. We observed that the BUN concentration was positively correlated with anti-SARS-CoV-2 spike antibody titers in hemodialysis patients after COVID-19 vaccination. However, the normalized protein catabolism rate—an indirect marker of dietary protein intake—was not associated with anti-SARS-CoV-2 spike antibody titers in hemodialysis patients in our study. The BUN concentration was reported to be affected by various factors, including the catabolic state, gastrointestinal bleeding, corticosteroid therapy, and dietary protein intake [12]. These factors might have influenced our present findings. Further studies are required to clarify whether dietary protein intake is associated with the anti-SARS-CoV-2 spike antibody response after COVID-19 vaccination in hemodialysis patients.
Many studies have reported that age was negatively associated with the anti-SARS-CoV-2 spike antibody response in hemodialysis patients [4,5,6, 13, 14]. However, in the present study, age was not associated with the anti-SARS-CoV-2 spike antibody titer in hemodialysis patients. Several reasons might explain the discrepancy between our results and those of previous studies. First, previous studies analyzed Caucasian patients, whereas our study involved Japanese patients. Therefore, the difference in ethnicity might have affected our results. Second, we conducted multiple linear regression analyses that used more covariates, including hemoglobin and BUN, compared with previous studies. These covariates might have influenced our results. Further studies incorporating different ethnicities and other covariates are necessary to clarify the influence of age on the anti-SARS-CoV-2 spike antibody response in hemodialysis patients.
In the present study, anti-SARS-CoV-2 spike antibody titers were measured 4 weeks after the second dose of the COVID-19 vaccine. In most studies that investigated factors associated with the anti-SARS-CoV-2 spike antibody response, the anti-SARS-CoV-2 spike antibody titer was measured between 3 and 6 weeks after the second dose of the COVID-19 vaccine [4, 5, 13,14,15]. However, one study reported that the anti-SARS-CoV-2 spike antibody titers in hemodialysis patients started to increase more slowly compared with those in healthy controls and continued to rise 5 weeks after the second dose of the COVID-19 vaccine [6]. Further studies are necessary to determine the optimal timing of anti-SARS-CoV-2 spike antibody response measurements for hemodialysis patients. In our study, the age of hemodialysis patients was 71.4 ± 12.2 years, and that of healthy controls was 48.5 ± 14.4 years. Most previous studies that compared the anti-SARS-CoV-2 spike antibody response between hemodialysis patients and healthy controls had a considerable difference in age between the two groups (approximately 70 years vs. approximately 50 years) [13,14,15]. Therefore, studies with an appropriate age-matched control group are warranted to assess the anti-SARS-CoV-2 spike antibody response in hemodialysis patients.
This study had several limitations. First, it was conducted with a relatively small number of patients (n = 75) from a single center, which might have reduced the statistical power to detect significance. Second, all participants were Japanese patients from a single center, which might limit the generalizability of our study findings. Third, the possibility that asymptomatic COVID-19-infected patients might have been included in this study cannot be excluded, although we did not include patients who were suffering from COVID-19. Fourth, the anti-SARS-CoV-2 spike antibody titer measured before a second COVID-19 vaccination was reported to be positively correlated with the anti-SARS-CoV-2 spike antibody titer obtained after the second COVID-19 vaccination in patients without renal impairment [16]. However, we did not investigate the influence of the anti-SARS-CoV-2 spike antibody titer determined before the second COVID-19 vaccination in this study, because the patients’ anti-SARS-CoV-2 spike antibody titer was not measured before their second COVID-19 vaccination. Therefore, large-scale, multicenter, and multiethnic studies are needed to validate our present findings.
In conclusion, autoimmune disease presence, lymphocyte counts, hemoglobin levels, and BUN concentrations were associated with the anti-SARS-CoV-2 spike antibody titer in Japanese patients undergoing hemodialysis after they received the second dose of the COVID-19 vaccine.
References
Bergwerk M, Gonen T, Lustig Y, Amit S, Lipsitch M, Cohen C, et al. Covid-19 breakthrough infections in vaccinated health care workers. N Engl J Med. 2021;385(16):1474–84. https://doi.org/10.1056/NEJMoa2109072.
Kageyama T, Ikeda K, Tanaka S, Taniguchi T, Igari H, Onouchi Y, et al. Antibody responses to BNT162b2 mRNA COVID-19 vaccine and their predictors among healthcare workers in a tertiary referral hospital in Japan. Clin Microbiol Infect. 2021. https://doi.org/10.1016/j.cmi.2021.07.042.
Vassilaki N, Gargalionis AN, Bletsa A, Papamichalopoulos N, Kontou E, Gkika M, et al. Impact of age and sex on antibody response following the second dose of COVID-19 BNT162b2 mRNA vaccine in greek healthcare workers. Microorganisms. 2021. https://doi.org/10.3390/microorganisms9081725.
Grupper A, Sharon N, Finn T, Cohen R, Israel M, Agbaria A, et al. Humoral response to the Pfizer BNT162b2 vaccine in patients undergoing maintenance hemodialysis. Clin J Am Soc Nephrol. 2021;16(7):1037–42. https://doi.org/10.2215/CJN.03500321.
Bachelet T, Bourdenx JP, Martinez C, Mucha S, Martin-Dupont P, Perier V, et al. Humoral response after SARS-CoV-2 mRNA vaccines in dialysis patients: integrating anti-SARS-CoV-2 spike-protein-RBD antibody monitoring to manage dialysis centers in pandemic times. PLoS ONE. 2021;16(10): e0257646. https://doi.org/10.1371/journal.pone.0257646.
Van Praet J, Reynders M, De Bacquer D, Viaene L, Schoutteten MK, Caluwe R, et al. Predictors and dynamics of the humoral and cellular immune response to SARS-CoV-2 mRNA vaccines in hemodialysis patients: a multicenter observational study. J Am Soc Nephrol. 2021. https://doi.org/10.1681/ASN.2021070908.
Shinzato T, Nakai S, Fujita Y, Takai I, Morita H, Nakane K, et al. Determination of Kt/V and protein catabolic rate using pre- and postdialysis blood urea nitrogen concentrations. Nephron. 1994;67(3):280–90. https://doi.org/10.1159/000187980.
Elkayam O, Paran D, Caspi D, Litinsky I, Yaron M, Charboneau D, et al. Immunogenicity and safety of pneumococcal vaccination in patients with rheumatoid arthritis or systemic lupus erythematosus. Clin Infect Dis. 2002;34(2):147–53. https://doi.org/10.1086/338043.
Elkayam O, Amir S, Mendelson E, Schwaber M, Grotto I, Wollman J, et al. Efficacy and safety of vaccination against pandemic 2009 influenza A (H1N1) virus among patients with rheumatic diseases. Arthritis Care Res. 2011;63(7):1062–7. https://doi.org/10.1002/acr.20465.
Ekiz C, Agaoglu L, Karakas Z, Gurel N, Yalcin I. The effect of iron deficiency anemia on the function of the immune system. Hematol J. 2005;5(7):579–83. https://doi.org/10.1038/sj.thj.6200574.
Bergstrom J. Nutrition and mortality in hemodialysis. J Am Soc Nephrol. 1995;6(5):1329–41. https://doi.org/10.1681/ASN.V651329.
Edelstein CL. Biomarkers of acute kidney injury. Adv Chronic Kidney Dis. 2008;15(3):222–34. https://doi.org/10.1053/j.ackd.2008.04.003.
Yanay NB, Freiman S, Shapira M, Wishahi S, Hamze M, Elhaj M, et al. Experience with SARS-CoV-2 BNT162b2 mRNA vaccine in dialysis patients. Kidney Int. 2021;99(6):1496–8. https://doi.org/10.1016/j.kint.2021.04.006.
Paal M, Arend FM, Lau T, Hasmann S, Soreth-Rieke D, Sorodoc-Otto J, et al. Antibody response to mRNA SARS-CoV-2 vaccines in haemodialysis patients. Clin Kidney J. 2021;14(10):2234–8. https://doi.org/10.1093/ckj/sfab127.
Stumpf J, Siepmann T, Lindner T, Karger C, Schwobel J, Anders L, et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: a prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg Health Eur. 2021;9: 100178. https://doi.org/10.1016/j.lanepe.2021.100178.
Takeuchi M, Higa Y, Esaki A, Nabeshima Y, Nakazono A. Does reactogenicity after a second injection of the BNT162b2 vaccine predict spike IgG antibody levels in healthy Japanese subjects? PLoS ONE. 2021;16(9): e0257668. https://doi.org/10.1371/journal.pone.0257668.
Acknowledgements
We thank the medical staff of Mizue Yuai Clinic for their excellent medical care support. We thank Edanz Group (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Funding
This study was not supported by any funding source.
Author information
Authors and Affiliations
Contributions
KH and MS conceived and designed the study. TS and TO collected and analyzed the data. KH wrote the first draft of the manuscript. SO made critical revisions. YM approved the final version. All authors contributed to this manuscript and approved the final version for submission.
Corresponding author
Ethics declarations
Conflict of interest statement
The authors declare that no conflict of interest exists.
Ethical approval
This study was approved by the Ethical Committee of Mizue Yuai Clinic (MYC 2021–01) and carried out in accordance with the fundamental principles contained within the Declaration of Helsinki.
Informed consent
Written informed consent was obtained from all participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Hirai, K., Shimotashiro, M., Sonoda, T. et al. Factors associated with anti-SARS-CoV-2 spike antibody titers after a second BNT162b2 mRNA COVID-19 vaccination in Japanese hemodialysis patients. Clin Exp Nephrol 26, 925–932 (2022). https://doi.org/10.1007/s10157-022-02223-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-022-02223-y