
Abstract
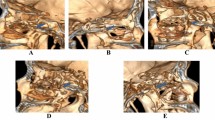
In retrosigmoid craniotomy, neurosurgeons usually depend on surface landmarks and their experience to evaluate the position of transverse-sigmoid sinus junction (TSSJ) and place an appropriate initial burr-hole, which is not accurate each time because of variability in different craniums. The authors introduce a simple procedure based on 3D computed tomography (CT) to localize the TSSJ in retrosigmoid craniotomy. Eighteen patients who underwent retrosigmoid craniotomy were analyzed. On the internal view of skull in 3D CT image, a simulative burr-hole was placed on the margin of transverse-sigmoid sinus groove junction. Then, on the external view of skull in 3D CT image, the center of the simulative burr-hole was marked and a coordinate system was established based on a line connected the digastric point and the asterion. Then the coordinate of the burr-hole’s center was measured in this coordinate system. In operation, the burr-hole was placed according to the coordinate measured previously and craniotomy was performed. The margin of TSSJ was exposed in each case. No damage of venous sinus was encountered. Post-operative skull base CT demonstrated a good match between the actual and predicted burr-hole and bone defects only existed along the cut line. This simple method could help in localizing the TSSJ and avoiding the risk of sinus injury and reducing the bone defect. It is sufficiently precise for practical application at surgical planning.








Similar content being viewed by others


References
Avci E, Kocaogullar Y, Fossett D, Caputy A (2003) Lateral posterior fossa venous sinus relationships to surface landmarks. Surg Neurol 59:392–397
Bozbuga M, Boran BO, Sahinoglu K (2006) Surface anatomy of the posterolateral cranium regarding the localization of the initial burr-hole for a retrosigmoid approach. Neurosurg Rev 29:61–63
da Silva E, Leal AG, Milano JB, da Silva L, Clemente RS, Ramina R (2010) Image-guided surgical planning using anatomical landmarks in the retrosigmoid approach. Acta Neurochir (Wien) 152:905–910
Day JD, Kellogg JX, Tschabitscher M, Fukushima T (1996) Surface and superficial surgical anatomy of the posterolateral cranial base: significance for surgical planning and approach. Neurosurgery 38:1079–1083
Day JD, Tschabitscher M (1998) Anatomic position of the asterion. Neurosurgery 42:198–199
Gharabaghi A, Rosahl SK, Feigl GC, Liebig T, Mirzayan JM, Heckl S, Shahidi R, Tatagiba M, Samii M (2008) Image-guided lateral suboccipital approach: part 1-individualized landmarks for surgical planning. Neurosurgery 62:18–22
Gharabaghi A, Rosahl SK, Feigl GC, Safavi-Abbasi S, Mirzayan JM, Heckl S, Shahidi R, Tatagiba M, Samii M (2008) Image-guided lateral suboccipital approach: part 2-impact on complication rates and operation times. Neurosurgery 62:24–29
Hamasaki T, Morioka M, Nakamura H, Yano S, Hirai T, Kuratsu J (2009) A 3-dimensional computed tomographic procedure for planning retrosigmoid craniotomy. Neurosurgery 64:241–245
Jia G, Wu Z, Zhang J, Zhang L, Xiao X, Tang J, Meng G, Geng S, Wan W (2010) Two-bone flap craniotomy for the transpetrosal-presigmoid approach to avoid a bony defect in the periauricular area after surgery on petroclival lesions: technical note. Neurosurg Rev 33:121–126
Lang JJ, Samii A (1991) Retrosigmoidal approach to the posterior cranial fossa. An anatomical study. Acta Neurochir (Wien) 111:147–153
Ojemann RG (2001) Retrosigmoid approach to acoustic neuroma (vestibular schwannoma). Neurosurgery 48:553–558
Raso JL, Gusmao SN (2011) A new landmark for finding the sigmoid sinus in suboccipital craniotomies. Neurosurgery 68:1–6
Ribas GC, Rhoton AL, Cruz OR, Peace D (2005) Suboccipital burr holes and craniectomies. Neurosurg Focus 19:E1
Tubbs RS, Loukas M, Shoja MM, Bellew MP, Cohen-Gadol AA (2009) Surface landmarks for the junction between the transverse and sigmoid sinuses: application of the “strategic” burr hole for suboccipital craniotomy. Neurosurgery 65:37–41
Ucerler H, Govsa F (2006) Asterion as a surgical landmark for lateral cranial base approaches. J Craniomaxillofac Surg 34:415–420
Yasargil MG (1996) Microneurosurgery. Thieme, New York
Financial support
Clinical specific projects from Beijing Municipal Science & Technology Commission (Z111107058811015)
Author information
Authors and Affiliations
Corresponding authors
Additional information
Comments
Mario Giordano, Hannover, Germany
In this well-illustrated technical note the authors report a method for preoperative and intraoperative localization of the transverse-sigmoid sinus junction using 3D computed tomography reconstruction and anatomical landmarks on the external surface of the skull. They use this procedure successfully in 18 retrosigmoid craniotomies for correct placement of the initial burr-hole.
The transverse and sigmoid sinuses are fundamental landmarks for retrosigmoid approach providing orientation for both craniotomy and dural opening. The overexposure is anyway unnecessary and their damage can lead to disastrous consequences for the patient. Therefore the idea of a coordinate-based system to localize the transverse-sigmoid sinus junction is interesting because of the well-known interpersonal variation of its anatomy.
This straightforward paper helps a better understanding of the correlation between superficial and intracranial structures, thus more publications of this type are needed to facilitate young neurosurgeons in their everyday practice.
Guilherme Carvalhal Ribas, São Paulo, Brazil
The current neuroimaging 3D reconstructions allow the neurosurgeon to plan ahead and even to simulate his procedures, taking already in consideration the patients’ individual important anatomical landmarks as their extracranial-intracranial bony relationships, their sulcal and gyral own pattern, the individual anatomy of their cisterns and ventricles, the actual position of arteries, veins and cranial nerves, and the relationships of all these structures with the lesion to be operated on. Further use of CT and MRI images’ fusion will definitely enhance this type of pre-operative information, putting together bone and intracranial structures.
In this direction Xia et al. propose in this article a straightforward and practical technical note about the important feature of localizing the transverse – sigmoid sinuses’ junction, which constitutes the main natural limit of the suboccipital exposures. Their method is simple considering the usually available CT facilities and is already based in a fair number of patients (18 cases).
Personally I believe that their findings are not significantly different of the previous related anatomical studies if we consider the statistical variations pertinent to the data obtained from cadaveric specimens. In a previous study we did we found that a 1 cm burr hole centered 1 cm anteriorly to the Asterion and with its superior base on the parietomastoid suture exposed the inferior aspect of the transverse-sigmoid sinuses’ junction in 84 % of the studied specimens (1, 2, 3), very much compatible with Xia et al. findings and illustrations.
Nevertheless this type of study definitely constitutes one step ahead of the usual anatomical studies since it is based in the patient’ own anatomy as provided by his own imaging data, and should be encouraged in order to generate more practical anatomical data able to take also into account unexpected anatomical variations.
References
1. Ribas GC. Study of the anatomic relationships of the lambdoid, occipitomastoid and parietomastoid sutures with the transverse and sigmoid sinuses, and of regional burr holes sites. São Paulo: Doctorship Thesis, Faculdade de Medicina da Universidade de São Paulo, 1991.
2. Ribas GC, Rhoton AL Jr, Cruz OR, Peace D. Temporo-parieto-occipital burr hole sites study and systematized approaches proposal. In: Samii M, editor. Skull base surgery, anatomy, diagnosis and treatment. Basel: Karger; 1994. p. 723–30.
3. Ribas GC, Rhoton AL Jr, Cruz OR, Peace D. Suboccipital burr holes and craniectomies. Neurosurg Focus 19(2):E1, 2005.
Rights and permissions
About this article
Cite this article
Xia, L., Zhang, M., Qu, Y. et al. Localization of transverse-sigmoid sinus junction using preoperative 3D computed tomography: application in retrosigmoid craniotomy. Neurosurg Rev 35, 593–599 (2012). https://doi.org/10.1007/s10143-012-0395-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-012-0395-0