
Abstract
Background
Management options for treatment of quadrigeminal arachnoid cysts (QAC) include microsurgical/endoscopic fenestration or shunt. There is an open debate about which method is the best. Microsurgical fenestration is well suited for treatment of QAC with predominant infratentorial component and without hydrocephalus making endoscopic procedures more challenging.
Method
We describe the microsurgical technique and related anatomy to fenestrate infratentorial QAC through supracerebellar infratentorial approach. We also discuss our experiences with this approach, some of the drawbacks and nuances.
Conclusion
Navigation-guided microsurgical fenestration of infratentorial QAC is the authors’ surgical approach of choice for treating these rare challenging lesions when not associated with hydrocephalus.




Similar content being viewed by others

References
Aboul-Enein H, El-Aziz Sabry AA, Hafez Farhoud A (2015) Supracerebellar infratentorial approach with paramedian expansion for posterior third ventricular and pineal region lesions. Clin Neurol Neurosurg 139:100–109
Cinalli G, Spennato P, Columbano L, Ruggiero C, Aliberti F, Trischitta V, Buonocore MC, Cianciulli E (2010) Neuroendoscopic treatment of arachnoid cysts of the quadrigeminal cistern: a series of 14 cases. J Neurosurg Pediatr 6(5):489–497
Ciricillo SF, Cogen PH, Harsh GR, Edwards MS (1991) Intracranial arachnoid cysts in children. A comparison of the effects of fenestration and shunting. J Neurosurg 74(2):230–235
Gangemi M, Seneca V, Colella G, Cioffi V, Imperato A, Maiuri F (2011) Endoscopy versus microsurgical cyst excision and shunting for treating intracranial arachnoid cysts. J Neurosurg Pediatr 8(2):158–164
Garg K, Tandon V, Sharma S, Suri A, Chandra PS, Kumar R, Mahapatra AK, Sharma BS (2015) Quadrigeminal cistern arachnoid cyst: a series of 18 patients and a review of literature. Br J Neurosurg 29(1):70–76
Hart MG, Santarius T, Kirollos RW (2013) How I do it–pineal surgery: supracerebellar infratentorial versus occipital transtentorial. Acta Neurochir (Wien) 155(3):463–467
Matsushima T, Rhoton AL Jr, de Oliveira E et al (1983) Microsurgical anatomy of the veins of the posterior fossa. J Neurosurg 59:63–105
Oliveira J, Cerejo A, Santos SP et al (2013) The infratentorial supracerebellar approach in surgery of lesions of the pineal region. Surg Neurol Int 4:154
Rhoton AL Jr (2000) Tentorial incisura. Neurosurgery 47:131–153
Rhoton AL Jr (2000) The posterior fossa veins. Neurosurgery 47:69–92
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
Not applicable.
Informed consent
Informed patient consent was obtained for the procedure illustrated.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
1 Microsurgical fenestration through SCIT, with the use of real-time neuronavigation-guided microscope, is well suited for treatment of QAC without hydrocephalus as far as these conditions make the execution of endoscopic procedures challenging.
2. The success rate reported in literature was almost similar after the microsurgical fenestration and the endoscopic procedure.
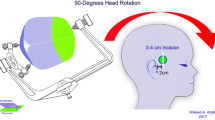
3. Concorde position is the senior author’s position of choice for this surgery. This position, with operating table in a minimal anti-Trendelenburg position and effective cisternal opening, allows an adequate cerebellar relaxation and avoids venous air embolism that is the major complication of the sitting and semi-sitting positions. Therefore, concorde position is an effective and safe position to approach the pineal region.
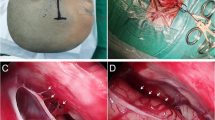
4. The exposure of the transverse sinus is important to provide a full access to the superior cerebellar surface.
5. Large and small QACs are usually associated with different anatomical conditions. The former is associated with a large surgical corridor and a distorted anatomy of surrounding venous and neural structures of the posterior fossa. In contrast, small QACs are usually associated with a narrow surgical corridor, limited deep veins exposure, and a substantially normal anatomy of the surrounding venous and neural structures.
6. The SCIT approach implies a long working distance that requires microsurgical expertise with the use of long microinstruments.
7. Small lateral bridging veins located along the trajectory of the surgical corridor can be sacrificed if necessary, during microscope dissection. On the contrary, the sacrificing of larger veins on the midline, such as superior vermian veins and precentral cerebellar vein, must be avoided.
8. Arachnoid band dissection and a wide opening of the AMQ are necessary to identify deep veins and their branches, thus avoiding injury to them. Therefore, an extensive knowledge of the deep veins anatomy is the cornerstone to achieve a safe QAC fenestration.
9. The microsurgical approach allows the surgeon to control the bleeding from deep veins promptly and easily when compared with endoscopic approach.
10. A wide fenestration of the cyst wall is important to ensure a free CSF flow from the cisterns into the cyst and to minimise the risk of recurrence.
This article is part of the Topical Collection on Neurosurgical technique evaluation
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 68689 KB)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Campagnaro, L., Bonaudo, C., Capelli, F. et al. Microscope neuronavigation-guided microsurgical fenestration of quadrigeminal cistern arachnoid cysts: how I do it. Acta Neurochir 165, 2561–2565 (2023). https://doi.org/10.1007/s00701-023-05531-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-023-05531-8