
Abstract
Background
As a pioneer center in the field of stereotaxy, Sainte-Anne school has always advocated the use of intraoperative imaging for stereotactic procedures to optimize both safety and accuracy. With the advent of intraoperative mobile CT unit, the robot-assisted stereotactic biopsy procedure has been recently updated.
Method
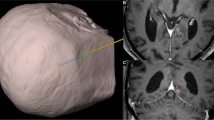
Herein, we aim at describing our new surgical procedure that combines robotic assistance (NeuroMate, Renishaw) and intraoperative cone beam CT imaging (O-Arm, Medtronic).
Conclusion
Intraoperative imaging with the O-Arm was efficiently incorporated into the workflow. This new equipment leads to optimizing operative time and an easier realization of intraoperative imaging.



Similar content being viewed by others


References
Daumas-Duport C, Szikla G, Vedrenne C (1979) [Stereotactic serial cerebral biopsies. Methodology (author’s transl)]. Arch Anat Cytol Pathol 27(3):135–139
Kajita Y, Nakatsubo D, Kataoka H, Nagai T, Nakura T, Wakabayashi T (2015) Installation of a NeuroMate robot for stereotactic surgery: efforts to conform to japanese specifications and an approach for clinical use—technical notes. Neurol Med Chir Tokyo 907–914
Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW (2016) The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol (Berl) 131(6):803–820
Pallud J, Varlet P, Devaux B, Geha S, Badoual M, Deroulers C, Page P, Dezamis E, Daumas-Duport C, Roux F-X (2010) Diffuse low-grade oligodendrogliomas extend beyond MRI-defined abnormalities. Neurology 74(21):1724–1731
Talairach J, Bancaud J, Bonis A, Tournoux P, Szikla G, Morel P (1961) Functional stereotaxic investigations in epilepsy. Methodological remarks concerning a case. Rev Neurol (Paris) 105:119–130
Zanello M, Roux A, Debacker C et al (2021) Postoperative intracerebral haematomas following stereotactic biopsies: poor planning or poor execution? Int J Med Robot Comput Assist Surg MRCAS 17(2):e2211
Zanello M, Roux A, Senova S et al (2021) Robot-assisted stereotactic biopsies in 377 consecutive adult patients with supratentorial diffuse gliomas: diagnostic yield, safety, and postoperative outcomes. World Neurosurg 148:e301–e313
Funding
This study was funded by the Nuovo-Soldati Foundation for Cancer Research scholarship, the Servier Foundation scholarship, and the Fundapro Foundation scholarship.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Patient consent
Informed consent was obtained from all individual participants included in the study.
Conflict of interest
The authors declare no competing interests.
Additional information
10 key points summary
1. Inform the patient about the time required to obtain definitive histomolecular diagnosis.
2. The planning of the stereotactic trajectory is a key step and requires time and attention (the planification is therefore best performed the day prior to surgery and ideally by two neurosurgeons).
3. Robotic assistance has many advantages over frame-based procedures including high mechanical accuracy, and it is less prone to human error (no reading and manual settings of the target coordinates).
4. Intraoperative imaging ensures the highest possible accuracy for a biopsy trajectory and makes it possible to know precisely the sites where the samples are taken for postoperative analyses.
5. General anesthesia precludes any high blood pressure episode.
6. The head should be firmly fixed using a head clamp.
7. Robot tool holder should be approached very close and ideally come in contact with the skin surface when drilling to avoid the potential bending of the drill bit and minimize mechanical inaccuracy.
8. Drilling of the skull should be smooth and slow, followed by coagulation of the dura, and measurement of the biopsy cannula based on the imagery.
9. The biopsy cannula is to be inserted with closed side cutting windows and subsequently opened once in the biopsy site, to perform a minimum of 10-s-long suction in order to obtain biopsy samples of a substantial size.
10. Several biopsy samples from different imaging components of the targeted lesion are to be obtained (the number of biopsy samples is not associated with increased morbidity).
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Brain Tumors
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 80038 kb)
Rights and permissions
About this article

Cite this article
Zanello, M., Simboli, G.A., Carron, R. et al. MRI-based and robot-assisted stereotactic biopsy with intraoperative CT imaging. Acta Neurochir 164, 3311–3315 (2022). https://doi.org/10.1007/s00701-022-05271-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-022-05271-1