
Abstract
Aims
To assess body composition by means of BOD POD in the large cohort of Italian Olympic athletes of many sport disciplines (studied at the same time), and to provide possible reference values for body composition in elite athletes.
Methods
1556 elite athletes, who took part in the selection procedure for the 2016 Rio Olympic Games for the National Italian Olympic Committee (CONI), were retrospectively studied. Body composition was determined using air plethysmography-based BOD POD.
Results
We observed that Fat Mass (FM) and Fat-free Mass (FFM) should be considered as two mutually independent domains in elite athletes. By performing Principal Component Analysis, we defined two independent main domains (respectively, representing FM and FFM), which presented different trends according to gender and static or dynamic exercise load. Lastly, we reported possible reference values for FM index and FFM index, respectively, representing the largest contributors to FM domain and FFM domain, and calculated as FM or FFM (kg)/height (m2).
Conclusions
Our findings might provide a basis to optimize the practical approach to body composition in athletes, highlighting the importance of considering indicators of fat mass and lean mass “simultaneously” and not specularly, according to different sport disciplines as well. Moreover, these data might contribute to standardize reference values for body composition in elite athletes, with a view to potentially helping to monitor and guide training regimens, prevent related detrimental practices and plan cardiometabolic prevention and rehabilitation programs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In the setting of metabolic assessment, body composition represents a key parameter that should never be overlooked, being hierarchically superior to body mass index (BMI) in predicting disease risk [1]. However, focus on body composition rather than body weight still represents a crucial cultural challenge, especially in elite athletes [2, 3]. In particular, Olympic athletes represent a unique subset among top sport performers, since they follow tough training regimens in order to gain the first position on the world podium every fourth year. Along with multiple other factors (optimal physical training, psychological and autonomic regulation) [4], assessment of body composition may indeed help to monitor the quality of training regimens in order to ultimately optimize competitive performance, according to the specific sport discipline [5, 6].
Despite strong evidence for the importance of body composition in elite athletes, universally applicable reference values are to date still lacking. Several studies have been previously performed in this context [2, 5,6,7,8,9,10,11], featuring nonetheless a wide range of limitations, such as small sample size, enrollment of non-elite athletes, ethnic variability, issues with assessment methods (in terms of heterogeneity, reliability, invasiveness) and/or evaluation timing (in- or off-season training period).
Goal of the present study was to assess body composition by means of BOD POD in the large cohort of Italian Olympic athletes of many sport disciplines, studied at the same time, with a view to providing possible reference values for body composition in elite athletes.
Methods
Study population and methodology
This retrospective observational study involved data from 1556 elite athletes (99.2% of Caucasian ethnicity) (888 males and 668 females) (age 23.9 [19.6–28.6] and 22.6 [18.8–27.1], respectively) who took part in the selection procedure for the 2016 Rio Olympic Games for the National Italian Olympic Committee (CONI) [12]. All athletes were cleared for active sport participation. Thus, they were free from evidence of disease that could interfere with results. The assessment procedure took place at the Institute of Medicine and Sport Science (CONI, Rome), as part of the preparticipation screening, while data analysis was performed at the Exercise Medicine Unit, Istituto Auxologico Italiano, IRCCS, University of Milan.
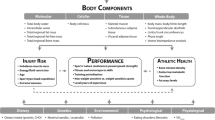
The whole cohort was subdivided into nine groups according to Mitchell classification of sports disciplines [13], based on peak static and dynamic loads achieved during competition (Fig. 1).

Classification of sports disciplines based on peak static and dynamic components achieved during competition (adapted from [13]). A progressive number (1–9) was given to each sport category. The increasing dynamic component is related to the estimated percentage of maximal oxygen uptake (VO2max) reached and results in an increasing cardiac output. The increasing static component is related to the estimated percentage of maximal voluntary contraction reached and results in an increasing blood pressure load. LD = low dynamic load; MD = moderate dynamic load; HD = high dynamic load; LS = low static load; MS = moderate static load; HS = high static load
Body composition was determined using air plethysmography-based BOD POD (Life Measurements Inc., Concord, CA, USA) according to the procedures recommended by the manufacturer [14, 15]. This noninvasive methodology was validated against other well recognized methods [16,17,18] in general adult and pediatric population as well as in athletes [2, 19,20,21]. Indeed, it was employed in many scientific papers in order to assess body composition as well as change in body composition after different training protocols both in athletes [19, 22,23,24,25,26] and non-athletes healthy subjects [27, 28]. The athletes were measured after at least 8 h of rest. When it was impossible to respect the 8 h of rest, the athlete was measured at least 2 h away from the ergometric test. Prior to each test, the BOD POD was calibrated according to the manufacturer’s instructions. While wearing minimal clothing (spandex shorts, swimsuit or tight-fitting underwear) and a swim cap, each subject was weighed on a calibrated digital scale to the nearest 20 g. The subject was then seated within the Air Displacement Plethysmography chamber for 2 measures of body volume, each lasting approximately 35–45 s. If the first 2 body volume values did not agree within 150 ml, a third body volume measure was taken. If 2 of the 3 measures were not consistent, the system was recalibrated and the test was repeated. Regarding the Thoracic Gas volume, we used predicted values, according to the standard predictor equation based on age, gender and height provided by the software [29]. The BOD POD was sealed and the participant breathed normally for 35–40 s while BV was measured. In stable resting conditions two measurements were obtained, and their average was utilized to provide body volume (BV, l) and body mass (BM, kg), as well as derive % fat mass (FM) and % fat-free mass (FFM) with specific equations (Siri, Brozek, Ortiz, Lohman, Schutte), according to ethnicity, gender and age.
In order to normalize the values of athletes’ FM and FFM for height, Fat Mass Index (FMi) and Fat-free Mass Index (FFMi) were considered [30] and calculated as follows:
-
\({\text{FMi}} = {\text{FM}}\left( {{\text{kg}}} \right)/{\text{height}}\left( {{\text{m}}^{{2}} } \right)\)
-
\({\text{FFMi}} = {\text{FFM}}\left( {{\text{kg}}} \right)/{\text{height}}\left( {{\text{m}}^{{2}} } \right)\)
The present study was performed in according to the principles of Declaration of Helsinki and Title 45, US Code of Federal Regulations, Part 46, Protection of Human Subjects, Revised November 13 2001, effective December 13 2001, and was cleared by local Institutional Science Committee (Istituto Medicina e Scienza dello Sport, Roma) and by Ethics Committee of University of Milan (report dated 23 September, 2019). The study protocol was guided by the STROBE statement [31].
Statistical analysis
Continuous variables were presented as median (interquartile range). Categorical variables were presented as counts and percentages.
To visualize the shape of the distribution of the continuous variable analyzed, a nonparametric kernel density estimation method of the density function was applied, representing it by means of violin plots. The graphs were grouped by gender. This method allowed us to control whether specific patterns in the distributions of the variables were present. An examination of the summary statistics and boxplots would not highlight these patterns sufficiently.
As a preliminary step, to control for possible nonlinear non-monotonic associations between the variables studied, pairwise scatterplots and Pearson correlation coefficients were computed.
To jointly study the potential association between the anthropometric characteristics of the athletes, a principal component analysis (PCA) was performed.
This method allowed us to reduce the dimensionality of the dataset while preserving as much of the data variation as possible. This method consists of rotating the axes of the multivariate space of the original variables along orthogonal directions of maximal variance (principal components, PCs), and creating a new space defined by the PCs. Each of the PCs is characterized by a percentage of explained variance of the data. If a relevant amount of variance is explained by the first PCs, the projection of the variables as vectors on the subspace defined by the new axes can be useful in exploring correlation structures present in the data. If two variables are strongly correlated, they are projected close together (the correlation is positive) or conversely with maximum alignment (the correlation is negative). Otherwise, if they do not display correlation, they tend to be projected at an angle of 90 degrees. Moreover, if the subspace defined by the two principal components describes the variables well, these are projected toward a circle of radius unity, also known as the circle of correlation; otherwise, they tend to be projected close to the origin of the axes. In addition, it is possible to project individuals onto the new plane defined by the principal components to understand who shows similar multivariate patterns from those who show different ones.
By conducting this analysis, we tried to see how the nine Mitchell sports categories differentiate depending on the anthropometric variables studied. We analyzed the marginal trend of the first two principal components of each specific category by plotting the individual values of PC1 and PC2 versus the nine Mitchell sports categories and applying a nonparametric loess smoother. In line with the exploratory study objectives, no formal statistical testing was performed.
All the statistical analyses were conducted with R software (version 4.1.2).
Equity, diversity and inclusion statement
This study includes 888 males and 668 females athletes. They varied in gender, race and socioeconomic level. The authors are all Italian men and women, including 2 early career, 2 mid-career, 1 technician and 4 professors. The authors’ areas of expertise were exercise and sports medicine, endocrinology, internal medicine and behavioral medicine.
Results
Description of anthropometric variables
Table 1 reports the anthropometric variables of athletes stratified by gender. As expected, male athletes show greater values in all the variables except for FM, both in % and Kg, as compared to females.
Table 2 summarizes the anthropometric variables of athletes stratified by Mitchell sport category (Fig. 1).
Principal component analysis (PCA)
Considering the large number of parameters derived from body composition assessment, as well as the fact that some of them were mutually correlated, and that simple pairwise associations did not consider the joint relationships with the other variables, a thorough investigation of the association structure among the parameters was performed by exploiting principal component analysis (PCA). This was done to look at the amount of information (indicated by the proportion of variance explained by each principal component in %) that was carried by relevant experimental parameters. Starting from the entire set of data, PCA produced a smaller number of uncorrelated components. These components may suggest hypothesis about the nature of the modeling data structure, and attribute to groups of parameters a physiological meaning.
The principal component analyses were conducted for males and females separately.
The structure of correlation in the dataset considered the following variables: FMi and FFMi (derived from FM and FFM Kg, and height), FFM%, FM%, BD, BSA, BV, FM/FFM ratio, and age.
The cumulative proportion of variance explained by the first two principal components was 90%, so only these were thoroughly investigated.
While PC1 was characterized by FMi, FFM%, FM%, FM/FFM ratio, and BD variables, PC2 was characterized by FFMi, BSA, and BV variables. Figure 2 depicts the correlation structure of the data in females (A) and males (B) by projecting the variables in the space defined by the two dimensions. It is noteworthy that the variables FMi and FFMi form an angle of 90° degrees and so they seem uncorrelated. Moreover, the largest contributors for the characterization of PC1 and PC2 are FMi (22%) and FFMi (35%), respectively.

Considering the relevant amount of variance explained by the first dimensions, the projection of the variables as vectors on the subspace defined by the new axes can be useful in exploring their correlation structure. From the graph both for Females (A) and Males (B) FMi and FFMi do not display correlation, as they are projected at an angle of 90 degrees. Body density (bd) is inversely correlated with FMi but is not correlated with FFMi. As expected, BSA and Body Volume are highly correlated, as FMi and FM-FFM ratio (fmffm). Age is not well defined by PC1 and PC2 as its vector is closer to the origin
Since the nature of PCA requires that the dimensions extracted are uncorrelated with each other, and since FMi and FFMi are the largest contributors to PC1 and PC2, respectively, we could state that FMi and FFMi were mutually independent.
Figure 3 reports in two different scatterplots, both for females (A) and males (B), the trend of PC1 and PC2 values (including FMi and FFMi as the most representative variables, respectively) depending on the nine sport categories.

Trend of PC1 and PC2 values across the nine sport categories (according to Mitchell classification) in females (A) and males (B)
Regarding females (Fig. 3A), in disciplines with a low dynamic load (LD, cat 1, 2, 3, see Fig. 1), PC1 values decreased while PC2 values increased, as the static load increased. Instead, in categories with a moderate (MD, cat 4, 5, 6 see Fig. 1) and high dynamic load (HD, 7, 8, 9 see Fig. 1), the two PCs both increased, with the exception of category 5, which exhibited a significant decrease in both PC1 and PC2.
In males (Fig. 3B), the average values of PC1 decreased drastically in disciplines with a low dynamic load (LD, cat 1, 2, 3, see Fig. 1) from category 1 to 3 (as the static load increased), and then settled at low values up to category 9 (as the dynamic load increased). Notably, categories 6 and 9 were characterized by a slight increase in PC1 values, while the lowest average values were found in categories 5 and 7. PC2 steadily increased from category 1 to 3, reached maximum values in categories 4 to 6 (characterized by a moderate dynamic load), then it went down in category 7, and rose again as the static load increased.
Based on the above results—considering that FMi and FFMi are the largest contributors to PC1 and PC2, respectively, that they are mutually independent, and can be easily calculated in clinical practice—we tried to derive reference values for male and female elite athletes’ body composition according to sport discipline, with a view to monitoring and guiding training regimes of current and future athletes.
Table 3 summarizes average FMi and FFMi values in the nine sports categories. We observed that low static load (LS) disciplines are characterized by a decrease in FMi values with the increase in dynamic component (from Cat 1 to Cat 4, and Cat 7) both in males and females, while FFMi values remain substantially the same. Moderate static load (MS) disciplines are characterized by a different trend of FMi values, being lower in presence of moderate dynamic load (MD) (Cat 5) as compared to both low (LD) and high dynamic load (HD) (Cat 2 and Cat 8, respectively) both in males and females. On the contrary, FFMi values are similar across the three dynamic load levels in females and slightly higher in moderate dynamic load (MD) in males.
High static load (HS) disciplines are characterized by similar values of FMi across the three dynamic load levels (Cat 3, Cat 6, and Cat 9) in males, and by higher FMi values in moderate dynamic load (MD) disciplines (Cat 6) in females. Indeed, FFMi values in males are similar in low (LD) and high dynamic load (HD) categories and slightly higher in moderate dynamic load (MD) disciplines, while in females they are similar in moderate (MD) and high dynamic load (HD) categories and slightly lower in low dynamic load (LD) disciplines.
Discussion
In this paper, we assessed body composition by means of BOD POD in a large cohort of Olympic athletes of many sport disciplines studied at the same time, and we observed that FM and FFM should be considered as two mutually independent domains in elite athletes. By performing Principal Component Analysis, we defined two independent main domains (respectively, representing FM and FFM), which show different trends according to gender and static or dynamic exercise load. Lastly, we reported possible reference values for FMi and FFMi, representing the largest contributors to FM domain and FFM domain, respectively.
Body composition plays a crucial role in elite athletes, and improvements in body composition have been found to enhance both cardiorespiratory fitness and strength [6]. Notably, body composition is also related to the risk of eating disorders and unhealthy weight management practices, which are oft due to widespread unawareness and misperception, leading to extremes in underweight or—to a lesser extent—overweight, especially among weight sensitive sports performers [3]. In this respect, it is worth mentioning the female athlete triad (isolate or combined presence of amenorrhea, impaired bone mass, and eating disorders), with each component existing on a spectrum from optimal health to disease. This condition, arising from low energy availability, mainly affects girls practicing sports that require leanness [32, 33].
However, universally applicable reference values for body composition in elite athletes are to date still lacking. Several studies have been previously performed in this context [2, 5,6,7,8,9,10,11], featuring nonetheless a wide range of limitations, such as small sample size, enrollment of non-elite athletes, ethnic variability, issues with assessment methods (in terms of heterogeneity, reliability, invasiveness) and/or evaluation timing (in- or off-season training period). With particular regards to assessment of body composition, all the available techniques present some limitations. For instance, reliability of skinfold thickness measurement depends on the technician’s skill and the caliper’s brand; bioelectrical impedance analysis (BIA) is population-specific, it is influenced by multiple variables, and may underestimate/overestimate FFM; dual-energy X-ray absorptiometry (DXA) is highly reliable but expensive and associated with a small amount of radiation [16]. In this study, BOD POD was employed, which can be considered as the best noninvasive technology, allowing to obtain reasonably accurate measurement of essential elements of body composition (FM and FFM, both expressed in absolute physical units, kilograms, and nominal % value) [19, 34]. Based on air plethysmography, it is indeed simple, friendly, and somewhat inexpensive [2, 16]. Although disease states can affect its accuracy, this is not a concern for elite athletes, being free from evidence of disturbances. Notably, this methodology has been also validated in athletes [20, 21, 35], and well-employed to assess body composition as well as body mass changes after different training protocols both in athletes and general population [19, 22,23,24,25,26,27,28]. Further, it was even used as reference methodology to assess the validity and reliability of other new proposed techniques in athletes [36,37,38,39].
We observed, by employing advanced statistics, that two simple Indexes (FMi and FFMi) [30, 40,41,42,43] were the largest contributors to PC1 and PC2, respectively, representing FM domain and FFM domain. According to such findings, FMi and FFMi, easily calculated from noninvasive body composition assessment, might have a considerable potential in clinical practice.
Thus, we leveraged these two Indexes to analyze the trend of FM and FFM across the nine Mitchell sports categories. In particular, FMi looks higher in athletes who perform disciplines with low dynamic component (LD), such as riflery and archery, while FFMi was lower in the same athletes as compared to other disciplines. This mirrored trend of FM and FFM is not present in some of the other sport categories, where FM and FFM seem to be two separate domains with mutually independent trends in both genders. In particular, athletes from category 7 (e.g., long-distance running) present not only low FM but also relatively low absolute values of FFM; conversely, athletes from category 9 (e.g., canoeing) present not only high FFM but also a considerable amount of FM. This observation may be of particular interest from a clinical point of view in monitoring athlete’s body composition. While in general population FFM is usually derived as percentage difference from FM, this cannot be applied to many categories of elite athletes. In this setting, FM and FFM need in fact to be considered separately. On the contrary, in the usual clinical practice FM and FFM are considered as two specular variables, with the consequent risk of missing some important information that is indeed necessary to help athletes reach/maintain their optimal body composition. This approach could be particularly relevant in identifying and managing athletes—especially those who perform weight sensitive sports—with risk for eating disorders and unhealthy weight management practices, which are oft due to widespread unawareness and misperception, leading to extremes in underweight or—to a lesser extent—overweight [3]. The possibility to have reference values both for FMi and FFMi from a relatively large population of elite athletes of many sport disciplines may further give a contribution to this goal.
Clinical implications
Our findings might provide a basis to optimize the practical approach to body composition in athletes, highlighting the importance of considering indicators of fat mass and lean mass “simultaneously” and not specularly, according to different sport disciplines as well. Moreover, these data might contribute to standardize reference values for body composition in elite athletes according to sports disciplines. Assessment of body composition in athletes could potentially help to monitor and guide training regimens of current and future athletes as well as prevent related detrimental practices (identification of at-risk athletes). This latter aspect also could be prominent among non-elite athletes playing sports that tend to emphasize low body weight, and it could help to plan cardiometabolic prevention and rehabilitation programs.
Limitations
Firstly, we have neither data regarding all sport disciplines nor a sufficient number of athletes in some of them. Consequently, we must consider nine main sport categories as indicated by international classification [13]. Indeed, we present data on the largest population of elite athletes in Italy, assessed using the same methodology, by the same researchers and at the same training epoch. Secondly, the percentage of female and male athletes in some sport disciplines is different (for instance, we have no male athletes performing synchronized swimming).
Data availability
Data are available upon reasonable request. We do not upload the data, considering the paucity of subjects in some sport disciplines (elite athletes well known by the community), which may not guarantee privacy.
References
Fitzpatrick M (2014) The relationship between body mass index and percent body fat in masters level competitive athletes. Ithaca College Theses. Published Online First: 1 January 2014. https://digitalcommons.ithaca.edu/ic_theses/11 (accessed 27 Jan 2022)
Ackland TR, Lohman TG, Sundgot-Borgen J et al (2012) Current status of body composition assessment in sport: review and position statement on behalf of the Ad Hoc research working group on body composition health and performance, under the auspices of the I.O.C Medical commission. Sport Med 42:227–249. https://doi.org/10.2165/11597140-000000000-00000
Meyer NL, Sundgot-Borgen J, Lohman TG et al (2013) Body composition for health and performance: a survey of body composition assessment practice carried out by the ad hoc research working group on body composition, health and performance under the auspices of the IOC medical commission. Br J Sports Med 47:1044–1053. https://doi.org/10.1136/bjsports-2013-092561
Pagani M, Lucini D (2009) Can autonomic monitoring predict results in distance runners? Am J Physiol Hear Circ Physiol 296:H1721–H1722. https://doi.org/10.1152/ajpheart.00337.2009
Portal S, Rabinowitz J, Adler-Portal D et al (2010) Body fat measurements in elite adolescent volleyball players: correlation between skinfold thickness, bioelectrical impedance analysis, air-displacement plethysmography, and body mass index percentiles. J Pediatr Endocrinol Metab 23:395–400. https://doi.org/10.1515/jpem.2010.061
Santos DA, Dawson JA, Matias CN et al (2014) Reference values for body composition and anthropometric measurements in athletes. PLoS ONE 9:e97846. https://doi.org/10.1371/journal.pone.0097846
Dixon CB, Deitrick RW, Pierce JR et al (2005) Evaluation of the BOD POD and leg-to-leg bioelectrical impedance analysis for estimating percent body fat in national collegiate athletic association division III collegiate wrestlers. J Strength Cond Res 19:85–91. https://doi.org/10.1519/14053.1
Hirsch KR, Smith-Ryan AE, Trexler ET et al (2016) Body composition and muscle characteristics of division i track and field athletes. J Strength Cond Res 30:1231–1238. https://doi.org/10.1519/JSC.0000000000001203
Reale R, Burke LM, Cox GR et al (2020) Body composition of elite Olympic combat sport athletes. Eur J Sport Sci 20:147–156. https://doi.org/10.1080/17461391.2019.1616826
Bentzur KM, Kravitz L, Lockner DW (2008) Evaluation of the bod pod for estimating percent body fat in collegiate track and field female athletes: a comparison of four methods. J Strength Cond Res 22:1985–1991. https://doi.org/10.1519/JSC.0b013e318185f196
Castizo-Olier J, Irurtia A, Jemni M et al (2018) Bioelectrical impedance vector analysis (BIVA) in sport and exercise: systematic review and future perspectives. PLoS ONE 13:e0197957. https://doi.org/10.1371/journal.pone.0197957
Lucini D, Sala R, Spataro A et al (2018) Can the use of a single integrated unitary autonomic index provide early clues for eventual eligibility for olympic games? Eur J Appl Physiol 118:919–926. https://doi.org/10.1007/s00421-018-3822-2
Mitchell JH, Haskell W, Snell P et al (2005) Task force 8: classification of sports. J Am Coll Cardiol 45:1364–1367. https://doi.org/10.1016/j.jacc.2005.02.015
COSMED (2015) BOD POD gold standard body composition tracking system operator’s manual-P/N 210-2400 Rev. M-DCO 1765, COSMED USA, Inc., Concord, CA, USA
Urlando A, Dempster P, Aitkens S (2003) A new air displacement plethysmograph for the measurement of body composition in infants. Pediatr Res 53:486–492. https://doi.org/10.1203/01.PDR.0000049669.74793.E3
Aragon AA, Schoenfeld BJ, Wildman R et al (2017) International society of sports nutrition position stand: diets and body composition. J Int Soc Sports Nutr 14:1–19. https://doi.org/10.1186/s12970-017-0174-y
Noreen EE, Lemon PWR (2006) Reliability of air displacement plethysmography in a large, heterogeneous sample. Med Sci Sports Exerc 38:1505–1509. https://doi.org/10.1249/01.mss.0000228950.60097.01
Nuñez C, Kovera AJ, Pietrobelli A et al (1999) Body composition in children and adults by air displacement plethysmography. Eur J Clin Nutr 53:382–387. https://doi.org/10.1038/sj.ejcn.1600735
Farley A, Slater GJ, Hind K (2021) Short-term precision error of body composition assessment methods in resistance-trained male athletes. Int J Sport Nutr Exerc Metab 31:55–65. https://doi.org/10.1123/IJSNEM.2020-0061
Kraemer WJ, Torine JC, Silvestre R et al (2005) Body size and composition of national football league players. J Strength Cond Res 19:485–489. https://doi.org/10.1519/18175.1
Utter AC, Goss FL, Swan PD et al (2003) Evaluation of air displacement for assessing body composition of collegiate wrestlers. Med Sci Sports Exerc 35:500–505. https://doi.org/10.1249/01.MSS.0000053726.16625.D5
Moon JR, Tobkin SE, Costa PB et al (2008) Validity of the bod pod for assessing body composition in athletic high school boys. J Strength Cond Res 22:263–268. https://doi.org/10.1519/JSC.0b013e31815f60ce
Collins MA, Millard-Stafford ML, Sparling PB et al (1999) Evaluation of the BOD POD® for assessing body fat in collegiate football players. Med Sci Sports Exerc 31:1350–1356. https://doi.org/10.1097/00005768-199909000-00019
Fields JB, Metoyer CJ, Casey JC et al (2018) Comparison of body composition variables across a large sample of national collegiate athletic association women athletes from 6 competitive sports. J Strength Cond Res 32:2452–2457. https://doi.org/10.1519/JSC.0000000000002234
Heydenreich J, Kayser B, Schutz Y et al (2017) Total energy expenditure, energy intake, and body composition in endurance athletes across the training season: a systematic review. Sport Med Open 3:1–24. https://doi.org/10.1186/s40798-017-0076-1
Cook RA, Hastings B, Gottschall JS (2014) Time in 85–100% heart rate zone increases lean body mass and V02Max in NCAA division I soccer players. J Fit Res 3:12–18
Gillen JB, Martin BJ, MacInnis MJ et al (2016) Twelve weeks of sprint interval training improves indices of cardiometabolic health similar to traditional endurance training despite a five-fold lower exercise volume and time commitment. PLoS ONE 11:e0154075. https://doi.org/10.1371/journal.pone.0154075
Schoenfeld BJ, Aragon AA, Wilborn CD et al (2014) Body composition changes associated with fasted versus non-fasted aerobic exercise. J Int Soc Sports Nutr 11:1–7. https://doi.org/10.1186/s12970-014-0054-7
Mccrory MA, Molé PA, Gomez TD et al (1998) Body composition by air-displacement plethysmography by using predicted and measured thoracic gas volumes. J Appl Physiol 84:1475–1479. https://doi.org/10.1152/jappl.1998.84.4.1475
Kyle UG, Schutz Y, Dupertuis YM et al (2003) Body composition interpretation: contributions of the fat-free mass index and the body fat mass index. Nutrition 19:597–604. https://doi.org/10.1016/S0899-9007(03)00061-3
Von Elm E, Altman DG, Egger M et al (2007) The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Epidemiology 18:800–804. https://doi.org/10.1097/EDE.0b013e3181577654
Weiss Kelly AK, Hecht S (2016) The female athlete triad. Pediatrics. https://doi.org/10.1542/peds.2016-0922
George C, Leonard J, Hutchinson M (2011) The female athlete triad: a current concepts review. S Afr J Sport Med 23:50. https://doi.org/10.17159/2078-516x/2011/v23i2a354
Kerkhof PLM, Peace RA, Handly N (2019) Ratiology and a complementary class of metrics for cardiovascular investigations. Physiology 34:250–263. https://doi.org/10.1152/physiol.00056.2018
Houska CL, Kemp JD, Niles JS et al (2018) Comparison of body composition measurements in lean female athletes. Int J Exerc Sci 11:417–424
Ferri-Morales A, Nascimento-Ferreira MV, Ubago-Guisado E et al (2018) Agreement between standard body composition methods to estimate percentage of body fat in young male athletes. Pediatr Exerc Sci 30:402–410. https://doi.org/10.1123/pes.2017-0171
Wagner DR, Cain DL, Clark NW (2016) Validity and reliability of a-mode ultrasound for body composition assessment of NCAA division i athletes. PLoS ONE 11:e0153146. https://doi.org/10.1371/journal.pone.0153146
Cross P, Shim A, Verhulst A et al (2011) Assessing various body composition measurements as an appropriate tool for estimating body fat in division I female collegiate athletes. J Sci Med Sport 14:e93. https://doi.org/10.1016/j.jsams.2011.11.192
Devrim-Lanpir A, Badem EA, Işık H et al (2021) Which body density equations calculate body fat percentage better in olympic wrestlers?—comparison study with air displacement plethysmography. Life 11:707. https://doi.org/10.3390/life11070707
VanItallie TB, Yang MU, Heymsfield SB et al (1990) Height-normalized indices of the body’s fat-free mass and fat mass: potentially useful indicators of nutritional status. Am J Clin Nutr 52:953–959. https://doi.org/10.1093/AJCN/52.6.953
Schutz Y, Kyle UUG, Pichard C (2002) Fat-free mass index and fat mass index percentiles in Caucasians aged 18–98 y. Int J Obes Relat Metab Disord 26:953–960. https://doi.org/10.1038/SJ.IJO.0802037
Dulloo AG, Jacquet J, Solinas G et al (2010) Body composition phenotypes in pathways to obesity and the metabolic syndrome. Int J Obes (Lond) 34(Suppl 2):S4-17. https://doi.org/10.1038/IJO.2010.234
Takase M, Nakamura T, Hirata T et al (2022) Association between fat mass index, fat-free mass index and hemoglobin A1c in a Japanese population: the Tohoku medical megabank community-based cohort study. J Diabetes Investig 13:858–867. https://doi.org/10.1111/JDI.13729
Acknowledgments
The authors would like to acknowledge the staff and athletes who helped facilitate this research.
Funding
Open access funding provided by Università degli Studi di Milano within the CRUI-CARE Agreement. This research was partially funded by the Italian Ministry of Health, and the PON PhD scholarship.
Author information
Authors and Affiliations
Contributions
All authors have contributed to the study development, data analysis, and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This is a retrospective study based on the Olympic Athletes database of the Exercise Clinic (located at Istituto Auxologico Italiano) of the University of Milan. All data were obtained as part of the yearly preparticipation clinical evaluation of the Italian Olympic athletes national pool, and performed at the CONI Medical Institute in Rome. All athletes signed an informed consent not only to the clinical evaluation (necessary for their participation to the Olympic games) but also for eventual use of their anonymized data in future studies. This procedure has been approved by the scientific committee of the CONI Institute (17 April 2017) and the Ethics Committee of the University of Milano (23 September 2019).
Informed consent
All subjects gave their written informed consent.
Additional information
Managed by Massimo Federici.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Giovanelli, L., Biganzoli, G., Spataro, A. et al. Body composition assessment in a large cohort of Olympic athletes with different training loads: possible reference values for fat mass and fat-free mass domains. Acta Diabetol 61, 361–372 (2024). https://doi.org/10.1007/s00592-023-02203-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-023-02203-y