
Abstract
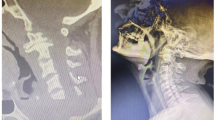
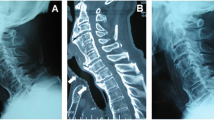
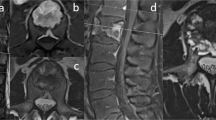
Anterior vertebral osteophytes and diffuse idiopathic skeletal hyperostosis (DISH) affecting the cervical spine are rare causes of dysphagia and dysphonia, and tend to affect aged patients. We report the case of a patient affected by DISH complaining of dysphagia and dysphonia due to massive osteophytosis of the anterior cervical spine. Spine X-ray films, direct laryngoscopy and esophagoscopy, cervical Magnetic Resonance Imaging were necessary to achieve a thoughtful characterisation of the osteophytic masses, and allowed the differential diagnosis with all the other causes of dysphagia and dysphonia. In absence of any effective medical therapy, surgery was required to relieve symptoms. Immediate clinical improvement occurred after the surgical resection of the osteophytes via an anterior cervical approach, without instrumented fusion. One and a half years after surgery, both clinical and radiological follow-up were negative for recurrence of the disease. In experienced hands, surgical treatment can be effective in resolve symptoms; instrumented fusion was not performed because, as found in this patient, disc degeneration in DISH is usually minimal or absent.
Résumé
L’ostéophyte vertébral antérieur et l’Hyperostose Squelettique Idiopatique Diffuse (DISH) affligeant le rachis cervical sont causes rares de dysphagie et de dysphonie et tendent à affecter les patients âgés. On rapporte le cas d’un patient atteint de DISH; il se plaint de dysphagie et de dysphonie qui sont dues au massif ostéophyte antérieur du rachis cervical. La radiographie du rachis cervical, la laryngoscopie et l’oesophagoscopie, la Résonance Magnétique Nucléaire cervicale étaient nécessaires pour arriver à une caractérisation complète des masses ostéophytiques et permettent aussi une différenciation de diagnostic avec les autres causes de dysphonie et de dysphagie. En absence d’une thérapie médicale efficace, la chirurgie était requérie pour soulager les symptômes. On a eu une immédiate amélioration clinique après la résection de l’ostéophyte par un abord cervical. Un an et demi après la chirurgie, l’analyse clinique et celle radiologique étaient toutes les deux négatives quant à la récidive de la maladie. en mains expérimentées, le traitement chirurgical peut être efficace pour soulager les symptômes; l’arthrodèse avec instrumentation n’est pas suffisante car, chez ces patients, la dégénérescence discale en DISH est en général minime voire absente.




Similar content being viewed by others
References
Barros Filho TE, Oliveira RP, Taricco MA, Gonzalez CH (1995) Hereditary multiple exostoses and cervical ventral protuberance causing dysphagia: a case report. Spine 20:1640–1642
Brandenberg G, Leibrock LG (1986) Dysphagia and dysphonia secondary to anterior cervical osteophytes. Neurosurgery 18:90–93
Forestier J, Rotes-Querol J (1950) Senile ankylosing hyperostosis of the spine. Ann Rheum Dis 9:321–330
Kissel P, Youmans JR (1982) Posttraumatic anterior cervical osteophyte and dysphagia: surgical report and literature review. J Spinal Disord 5:104–107
Krause P, Castro WHM (1994) Cervical hyperostosis: a rare cause of dysphagia. Case description and bibliographical survey. Eur Spine J 3:56–58
Mader R (2002) Clinical manifestations of diffuse idiopathic skeletal hyperostosis of the cervical spine. Semin Arthritis Rheum 32:130–135
Oga M, Mashima T, Iwakuma T, Sugioka Y (1993) Dysphagia complications in ankylosing spinal hyperostosis and ossification of the posterior longitudinal ligament: roetgenographic findings of the developmental process of cervical osteophytes causing dysphagia. Spine 18:391–394
Resnick D, Shapiro RF, Wiesner KB, Niwayama G, Utsinger PD, Shaul SR (1978) Diffuse idiopathic skeletal hyperostosis (DISH) [ankylosing hyperostosis of Forestier and Rotes-Querol]. Semin Arthritis Rheum 7: 153–187
Resnick D, Niwayama G (1998) Diffuse idiopathic skeletal hyperostosis. In: Resnick D, Niwayama G (eds) The diagnosis of bone and joint disorders, 2nd edn. WB Saunders Co, Ed, Philadelphia, pp 1562–1602
Yoskovitch A, Kantor S (2001) Cervical osteophytes presenting as unilateral cord paralysis and dysphagia. J Laryngol Otol 115:422–424
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Di Martino, A., Costa, V. & Denaro, V. Dysphagia and dysphonia due to anterior cervical osteophytes: report of a patient affected by DISH. Eur J Orthop Surg Traumatol 16, 344–347 (2006). https://doi.org/10.1007/s00590-006-0110-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-006-0110-3