
Abstract
Background
Due to increasing opportunities for abdominal imaging studies, bile duct stones are occasionally diagnosed without any symptoms. However, there has been no consensus on the management of asymptomatic bile duct stones. We conducted a retrospective longitudinal cohort study to investigate the natural history of asymptomatic bile duct stones and clinical outcomes according to the timing of endoscopic removal.
Methods
We identified consecutive patients who were diagnosed with asymptomatic common bile duct stones and categorized into those who were followed up with stones in situ (wait-and-see group) and those who received early endoscopic stone removal (intervention group). Cumulative incidence functions of biliary complications were estimated and compared between the groups.
Results
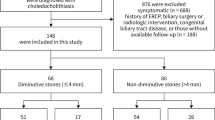
We included 191 patients (114 patients in the wait-and-see group and 77 patients in the intervention group). In the wait-and-see group, the cumulative incidence of biliary complications was 6.1% at 1 year, 11% at 3 years, and 17% at 5 years. Asymptomatic disappearance of stones was observed in 22 patients (19%). Procedure-related adverse events of early endoscopic stone removal of asymptomatic stones were observed in 25 (32%) patients including 4 (5.2%) with severe pancreatitis. The cumulative incidence function of biliary complications did not differ by treatment strategies (P = 0.55).
Conclusions
Biliary complications occurred in a substantial proportion of patients with asymptomatic bile duct stones, but early endoscopic removal appeared to have little effect on the prevention of further biliary complications. Given the risk of procedure-related pancreatitis, the wait-and-see strategy may become a management option of asymptomatic stones.


Similar content being viewed by others

References
Gigot J, Leese T, Dereme T, et al. Acute cholangitis. Multicariate analysis of risk factors. Ann Surg. 1989;209:435–8.
Tazuma S, Unno M, Igarashi Y, et al. Evidence-based clinical practice guidelines for cholelithiasis 2016. J Gastroenterol. 2017;52:276–300.
Williams E, Beckingham I, El Sayed G, et al. Updated guideline on the management of common bile duct stones (CBDS). Gut. 2017;66:765–82.
Committee ASOP, Maple JT, Ikenberry SO, et al. The role of endoscopy in the management of choledocholithiasis. Gastrointest Endosc. 2011;74:731–44.
Kondo S, Isayama H, Akahane M, et al. Detection of common bile duct stones: comparison between endoscopic ultrasonography, magnetic resonance cholangiography, and helical-computed-tomographic cholangiography. Eur J Radiol. 2005;54:271–5.
Freeman ML. Adverse outcomes of ERCP. Gastrointest Endosc. 2002;56:S273–S282282.
Cotton PB, Garrow DA, Gallagher J, et al. Risk factors for complications after ERCP: a multivariate analysis of 11,497 procedures over 12 years. Gastrointest Endosc. 2009;70:80–8.
Disario JA, Freeman ML, Bjorkman DJ, et al. Endoscopic balloon dilation compared with sphincterotomy for extraction of bile duct stones. Gastroenterology. 2004;127:1291–9.
Saito H, Kakuma T, Kadono Y, et al. Increased risk and severity of ERCP-related complications associated with asymptomatic common bile duct stones. Endosc Int Open. 2017;5:E809–E817817.
Kim SB, Kim KH, Kim TN. Comparison of outcomes and complications of endoscopic common bile duct stone removal between asymptomatic and symptomatic patients. Dig Dis Sci. 2016;61:1172–7.
Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010;71:446–54.
Miura F, Okamoto K, Takada T, et al. Tokyo guidelines 2018: initial management of acute biliary infection and flowchart for acute cholangitis. J Hepatobiliary Pancreat Sci. 2018;25:31–40.
Kiriyama S, Kozaka K, Takada T, et al. Tokyo guidelines 2018: diagnostic criteria and severity grading of acute cholangitis (with videos). J Hepatobiliary Pancreat Sci. 2018;25:17–30.
Yokoe M, Hata J, Takada T, et al. Tokyo guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2018;25:41–544.
Nakai Y, Kogure H, Yamada A, et al. Endoscopic management of bile duct stones in patients with surgically altered anatomy. Dig Endosc. 2018;30(Suppl 1):67–74.
Hakuta R, Hamada T, Nakai Y, et al. Multicenter retrospective and comparative study of 5-minute versus 15-second endoscopic papillary balloon dilation for removal of bile duct stones. Endosc Int Open. 2017;5:E1027–E10341034.
Takahara N, Isayama H, Sasaki T, et al. Endoscopic papillary balloon dilation for bile duct stones in patients on hemodialysis. J Gastroenterol. 2012;47:918–23.
Kawabe T, Komatsu Y, Tada M, et al. Endoscopic papillary balloon dilation in cirrhotic patients: removal of common bile duct stones without sphincterotomy. Endoscopy. 1996;28:694–8.
Itoi T, Ryozawa S, Katanuma A, et al. Japan Gastroenterological Endoscopy Society guidelines for endoscopic papillary large balloon dilation. Dig Endosc. 2018;30:293–309.
Hakuta R, Kawahata S, Kogure H, et al. Endoscopic papillary large balloon dilation and endoscopic papillary balloon dilation both without sphincterotomy for removal of large bile duct stones: a propensity-matched analysis. Dig Endosc. 2019;31:59–68.
Ozawa N, Yasuda I, Doi S, et al. Prospective randomized study of endoscopic biliary stone extraction using either a basket or a balloon catheter: the BasketBall study. J Gastroenterol. 2017;52:623–30.
Hamada T, Nakai Y, Isayama H, et al. Estimation and comparison of cumulative incidences of biliary self-expandable metallic stent dysfunction accounting for competing risks. Dig Endosc. 2014;26:270–5.
Kanda Y. Investigation of the freely available easy-to-use software 'EZR' for medical statistics. Bone Marrow Transplant. 2013;48:452–8.
Elmunzer BJ. Reducing the risk of post-endoscopic retrograde cholangiopancreatography pancreatitis. Dig Endosc. 2017;29:749–57.
Joyce W, Keane R, Burke G, et al. Identification of bile duct stones in patients undergoing laparoscopic cholecystectomy. Br J Surg. 1991;78:1174–6.
Moller M, Gustafsson U, Rasmussen F, et al. Natural course vs interventions to clear common bile duct stones: data from the Swedish Registry for Gallstone Surgery and Endoscopic Retrograde Cholangiopancreatography (GallRiks). JAMA Surg. 2014;149:1008–133.
Ammori BJ, Birbas K, Davides D, et al. Routine vs "on demand" postoperative ERCP for small bile duct calculi detected at intraoperative cholangiography. Clinical evaluation and cost analysis. Surg Endosc. 2000;14:1123–6.
Caddy G, Kirby J, Kirk S, et al. Natural history of asymptomatic bile duct stones at time of cholecystectomy. Ulster Med J. 2005;74:108–12.
Collins C, Maguire D, Ireland A, et al. A prospective study of common bile duct calculi in patients undergoing laparoscopic cholecystectomy: natural history of choledocholithiasis revisited. Ann Surg. 2004;239:28–33.
Yun SP, Seo HI. Clinical aspects of bile culture in patients undergoing laparoscopic cholecystectomy. Medicine (Baltimore). 2018;97:e11234.
Mazaki T, Mado K, Masuda H, et al. Prophylactic pancreatic stent placement and post-ERCP pancreatitis: an updated meta-analysis. J Gastroenterol. 2014;49:343–55.
Elmunzer BJ, Scheiman JM, Lehman GA, et al. A randomized trial of rectal indomethacin to prevent post-ERCP pancreatitis. N Engl J Med. 2012;366:1414–22.
Freeman ML, DiSario JA, Nelson DB, et al. Risk factors for post-ERCP pancreatitis: a prospective, multicenter study. Gastrointest Endosc. 2001;54:425–34.
Nakai Y, Isayama H, Tsujino T, et al. Cholecystectomy after endoscopic papillary balloon dilation for bile duct stones reduced late biliary complications: a propensity score-based cohort analysis. Surg Endosc. 2016;30:3014–20.
Tsujino T, Kawabe T, Komatsu Y, et al. Endoscopic papillary balloon dilation for bile duct stone: immediate and long-term outcomes in 1000 patients. Clin Gastroenterol Hepatol. 2007;5:130–7.
Author information
Authors and Affiliations
Contributions
RH, TH, and YN: conception and design of the study, analysis, and interpretation of the data, and drafting of the article. HO, SK, TS, TS, KI, KS, TS, NT, SM, HK, TW, TT, MT, OA, HI, and KK: critical revision of the article for important intellectual content. All authors: final approval of the article.
Corresponding author
Ethics declarations
Conflict of interest
We declare that we have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hakuta, R., Hamada, T., Nakai, Y. et al. Natural history of asymptomatic bile duct stones and association of endoscopic treatment with clinical outcomes. J Gastroenterol 55, 78–85 (2020). https://doi.org/10.1007/s00535-019-01612-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-019-01612-7