
Abstract
Context and objectives
The present study examined the perspectives of healthcare providers (HCPs) in designing a multi-disciplinary model of supportive cancer care for the relief of dermatology-related symptoms caused by monoclonal antibody therapies.
Methods
The study employed a mixed research methodology, with qualitative research embedded within a pragmatic prospective study of a registry protocol study. Patients undergoing oncology therapy with MoAB, anti-HER2, and anti-PD-L1 monoclonal antibodies were identified among a cohort of patients referred to an integrative oncology (IO) consultation for symptom relief and improved quality of life (QoL). Case studies with significant dermatology-related concerns were selected and presented to a panel of 6 HCPs trained in medical oncology, oncology nursing, family medicine, supportive cancer care, and IO. HCP narratives were qualitatively analyzed and assessed using ATLAS.Ti software for systematic coding.
Results
Of the 924 patients referred to the IO consultation, 208 were treated with monoclonal antibodies, from which 50 were selected for further evaluation. Of these, 7 cases were presented to the HCP team who were asked to identify treatment gaps requiring a multi-disciplinary approach. Qualitative analysis identified 3 major themes: a biophysical perspective; a psycho-social-spiritual perspective; and the implementation of integrated care.
Discussion
There is a need for a multi-disciplinary approach when treating patients suffering from monoclonal antibody treatment-related skin toxicities. HCP-reported themes highlight the need to identify patients for whom such an approach is warranted; conditions in which a psycho-social-spiritual perspective should be considered, in addition to a bio-physical approach; and considerations of who should be designated as the patient’s primary case manager.
Similar content being viewed by others


Introduction
The developing field of targeted immunotherapy has led to significantly better outcomes in the treatment of cancer. At the same time, these drugs have led to an increase in treatment-related dermatological symptoms such as acne, rashes, and itching [1]. Skin-related symptoms are frequently accompanied by emotional distress, with social and functional implications [2]. Immunotherapy-induced dermatological symptoms are increasingly being addressed by healthcare providers (HCPs), including oncology physicians and nurses, dermatologists, supportive cancer care professionals, family physicians, and others.
Many of today’s leading cancer centers provide complementary medicine within an evidence-based and integrative oncology (IO) setting, often as part of the center’s supportive care service [3]. The research supporting the impact of IO on symptom relief and quality of life (QoL) has led to the inclusion of many of these modalities in clinical practice guidelines of the American Society for Clinical Oncology (ASCO) and the European Society for Medical Oncology (ESMO), among others [4]. However, little has been published on the impact of IO on dermatological symptoms related to the use of immunotherapy drugs. The present study examined the extent to which monoclonal antibody treatment-related dermatological symptoms are being referred to IO services and qualitatively assessed a multi-disciplinary approach to treating these and related concerns. Recurrent themes were identified and analyzed, using the narratives of HCPs working in a patient-centered multi-disciplinary supportive care setting.
Methods
Study objectives
The primary study objective of the study was to explore the impact of a multi-disciplinary approach to the treatment of patients suffering from monoclonal antibody treatment-related skin toxicities, especially for conditions in which a patient-centered perspective may be required. Additional study objectives included identifying situations which require an HCP to be appointed as the patient’s case manager and whether a multi-disciplinary approach is perceived as necessary.
Study design and setting
The study employed a mixed research methodology, with qualitative research embedded within a pragmatic prospective study of a registry protocol study. The electronic files of patients participating in the study were searched for those receiving monoclonal antibody agents and who had been referred by their HCP to the IO service for the treatment of QoL-related indications. A qualitative analysis of 6 in-depth interviews with the oncology HCPs treating 7 of the identified patients was conducted, focusing on dermatological symptoms related to either the underlying cancer or to the monoclonal antibody drugs which the patients were taking during the IO consultation as part of their conventional cancer care. The predominant themes derived from these interviews were then identified and analyzed.
Patients participating in the prospective registry protocol study were recruited from August 2013 to February 2021 at the Oncology Service, Lin and Zebulon Medical Centers, Clalit Healthcare Services Haifa, Israel [5]. The two community-based oncology centers provide ambulatory oncology treatments, along with an IO service which offers patients a wide range of modalities addressing their QoL-related concerns. IO treatments are provided by a multi-disciplinary team of 6 integrative physicians (IPs), medical doctors trained in supportive cancer care and integrative medicine; 6 IO-trained nurses; 4 paramedical practitioners; and 6 integrative-medicine therapists, all with extensive training in integrative and supportive cancer care and with over 5 years of IO work experience.
Study population and IP consultation
Oncology patients aged ≥ 18 years and undergoing adjuvant, neo-adjuvant, or palliative oncology treatments for solid tumors were eligible for study inclusion. Patients who were unable to read or sign the informed consent form were excluded, as were patients with hemato-oncological disease. All patients require a structured referral to the IO consultation by one of their oncology HCPs, for at least one QoL-related indication (e.g., pain, nausea, itching). Following an initial IP consultation, in which the patient’s leading QoL-related concerns are addressed, treatment goals are co-defined with the patient, and an IO treatment plan is then co-designed.
Selection of patient files
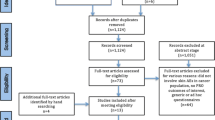
The files of eligible patients undergoing treatment with a monoclonal antibody drug, whether alone or in conjunction with other anti-cancer agents, were identified (Fig. 1). The agents being used included the MoAB (anti-EGFR monoclonal antibody) drug cetuximab; the anti-HER2 monoclonal antibody agent pertuzumab; and the anti-PD-L1 monoclonal antibody drugs nivolumab and pembrolizumab. Patients who reported dermatological symptoms, as mentioned in the patient file by one of their treating HCPs, were selected for further analysis. In total, 7 files were selected for qualitative analysis, this in light of the large amount of clinical data and diverse spectrum of dermatological-related concerns (Table 1). A panel of 6 HCPs (JL, OG, RDG, KS, YT, and MG) was then asked to read all of the 7 selected patient files and then interviewed by the first author (D.K.). Panel members were physicians working in oncology, dermatology, integrative medicine, family medicine, and supportive cancer care, and each was asked to reflect (providing feedback within a written narrative) on each of the 7 patient cases, while considering the following 6 questions:

Selection of patient files for analysis
-
1.
To the best of your knowledge, are the patient's skin-related symptoms a direct result of the monoclonal antibody drug?
-
2.
How would you advise the patient if you were asked for your help? What approach or treatment/s would you employ?
-
3.
Which of the other team members would you approach to help you treat the patient’s dermatological symptoms?
-
4.
For which of the following dermatological-related symptoms would you reach out to an HCP from another medical specialization? Who are the HCPs to whom you would turn to for this purpose?
-
5.
How would you prioritize the treatment of dermatological toxicities in patients who suffer from other, often debilitating symptoms and toxicities as well?
-
6.
Do you think that the patient's dermatological symptoms may have a negative effect on adherence to the conventional oncology treatment regimen? Should the goal of the IO treatment program be limited to relief of symptoms and improved QoL? Or should it include increasing adherence to the conventional oncology treatment regimen as well?
Qualitative analysis of the HCP narratives was conducted systematically using ATLAS.Ti Scientific Software (V.8). A qualitative content analysis was performed using a conventional content analysis approach, thereby avoiding the need for pre-established categories for coding [6]. Narratives relating to the identified codes were then sorted into categories and grouped into meaningful clusters, identifying emerging themes.
Results
Characteristics of study groups
The IO registry protocol database consisted of the electronic files of 924 oncology patients, of which 208 (22.51%) were being treated with monoclonal antibody drugs. The median age of the cohort was 60 years, and the majority of which were female (152, 73%) and listed Hebrew as their primary language (139, 66.8%). There was a wide variety of primary cancer sites (breast, 99; gastro-intestinal, 37; lung, 23; gynecological, 18), and most patients had a diagnosis of advanced disease (121, 58.2%). The most frequently used monoclonal antibody drugs were the MoAB (anti-EGFR monoclonal antibody) agent cetuximab; the anti-HER2 monoclonal antibody agent pertuzumab; and the anti-PD-L1 monoclonal antibody drugs nivolumab and pembrolizumab. A total of 14 patients reported dermatological-related symptoms which were attributed to the use of these drugs.
Identified themes
Qualitative content analysis of the HCP narratives yielded a number of codes which could be sorted into categories and clusters, with the identification of the following 3 major thematic groupings: a biophysical perspective; a psycho-social-spiritual perspective; and implementation of integrated care.
Theme I: bio-physical perspective
The first theme identified from the narratives of the panel of HCPs addressed a comprehensive bio-physical perspective of monoclonal antibody treatment-related dermatological symptoms. The study dermatologist differentiated between localized (simple) and systemic (complicated) dermatological effects of the drugs, pointing out the tendency to over-diagnose these effects.
I see many oncology patients with dermatological conditions that are not related to their oncology treatment. And even for those cases where the link between symptom and drug is clear, I am often reluctant to stop the oncology treatment, because of the implications regarding the patient’s disease.
The dermatologist’s approach was one of an open discussion with the patient, starting prior to and continuing throughout the treatment period. This approach was also evident in the oncology nurse’s narrative, which addressed strategies for preventing or reducing skin-related toxicities of the drugs. The supportive care physician, much like the dermatologist, first looked for other causes for the patient’s skin symptoms, which were not necessarily related to the monoclonal antibody drug being administered:
-
First, you’ll think of anything that can be treated and that is reversible. You’d like to check if she’s taking any other herbs or supplements which can cause rashes…. And then you want to make sure that this rash doesn’t look like anything that could be related to the disease.
All of the participating HCPs addressed the need for a multi-disciplinary and inter-disciplinary approach, as well as looking beyond the skin condition “per se.” The nurse addressed behavioral aspects; the supportive care physician suggested dietary changes and the use of pro-biotic products; and the integrative physician considered the use of acupuncture and anthroposophic medicine to reduce dermatological symptoms and address emotional distress.
Theme II: psycho-social-spiritual perspective
The second theme identified from the narratives of the HCP panel addressed a psycho-social-spiritual perspective, recognizing effects of the dermatological symptoms which extended beyond their physical manifestation. The dermatologist approached this theme using a metaphor of “widening” the biophysical diagnostic “borders” of the skin lesion, emphasizing the importance of effectively communicating with the patient on what they were experiencing and how they were coping.
It’s very important to be alert regarding the emotional impact on the patient...on her faith in her body. There is a tragedy here, and it requires the involvement of a social worker for emotional support. It’s not something you can deal with on your own. The scariest thing is that they lose faith in their body, in themselves.
The emotional aspects of the symptoms, as well as the patient’s relationship with their partner, were the focus of the nurse’s narrative. The family doctor’s narrative also addressed the psycho-social-spiritual perspective of patient care, taking into consideration the effectiveness of treatment within the emotional response, especially with respect to how the patient’s skin condition related to their role within the family and society, including their sexual identity and role as caregiver:
-
I ask the patient about whether her skin condition has an effect on her sexual role, her self-image. If she agrees, then I would ask her partner how he sees it; and how he thinks she feels about it…I would also talk with other family members. It really depends on the woman…she could be of a strong character, with many resources, and then it might be easier for her. But she could also suffer from depression, or a poor relationship with her partner…it affects everyone differently.
The integrative physician emphasized the importance of the relationship between dermatological symptoms related to the oncology treatment and depression, as well as the patient’s general QoL:
-
Metastases and skin-related symptoms can severely impair quality of life, and may lead to an avoidant personality (doesn’t want to leave home, doesn't meet with friends or family), and even depression. It’s as if it constantly reminds them that they are a cancer patient.
In this narrative, the integrative physician also addressed the need for compassion, which may be difficult in light of the unpleasant appearance of and sometimes strong odor from the patient’s skin condition:
-
Even if there is an off-putting feeling, talking about it makes it normal …It’s not something to be embarrassed about. Ask her about how much it bothers her, how it bothers her relationship with her partner…
The supportive care physician’s narrative addressed her specialty in family medicine, with extensive training in integrative medicine. In her opinion, the psycho-social aspects of the dermatological symptoms were primarily a function of the patient’s health-belief model:
-
It’s really trying to understand the person’s belief system. You need to find a way to engage them in a way that’s therapeutic. Sometimes you’ll meet somebody and he’ll show you his rash, but that’s only two minutes of the consultation…and then for the other 58 minutes I’ll take the person’s history and ask about their main concerns. The symptom that gets the patient through the door, opens the way to treat the whole person. If people are anxious or in distress, often the first thing would be a massage or a reflexology treatment. Engaging people, touching their skin very early on is helpful.
Theme III: implementation of integrated care
While the need for inter-disciplinary communication was emphasized by all of the panel HCPs in their narratives, the question of who is responsible for the patient’s care varied, as well as the need to ensure continuity of care. The dermatologist considered herself a counselor, with the oncologist as the case manager. The oncology nurse saw her role as that of a “case manager,” the most readily available HCP responsible for the patient’s QoL:
-
This [the patient’s trust in the medical team] is the most important challenge facing nurses; from the first meeting with the patient…it is our responsibility not to “brush off” the patient…the way it is done is that there is one doctor, one nurse…to make it clear to the patient that they have come to the right place…that they are in good hands.
All narratives addressed the need for a multi-disciplinary model of care based on effective communication. The dermatologist recommended including a psychologist in the team, as well as nurses and therapists to treat mouth sores. The oncologist emphasized the role of the social worker and the oncology nurse. The family physician referred patients to the oncologist, to the dermatologist, and to the integrative physician. The supportive care physician considered referring the patient to the psycho-oncologist, as well as to the team of IO practitioners for touch therapy, acupuncture, yoga, and mindfulness treatments. The collaboration within the multi-disciplinary team referred to both design and implementation of the patient-tailored treatment program:
-
Once a week there’s a meeting of my integrative team for one hour, where we discuss “difficult” patients…I present patients I have seen or that have changed their status, and we discuss them. I am the “bridge” between my team and the oncology team, as well as the family physician and community clinic nurse.
In contrast, the integrative physician pointed out barriers to the multi-disciplinary teamwork, specifically regarding patients with skin-related concerns:
-
The oncology team does not refer enough of their patients suffering from skin conditions to our service. At the same time, we as an integrative medicine team are often not as aware of dermatological symptoms as we are of other conditions, such as chemotherapy-induced peripheral neuropathy…it's not sufficiently embedded in our lexicon…I do not ask my patients enough about skin-related symptoms…
At the same time, she admitted that she does not usually address dermatological complications related to monoclonal antibody drugs, or to patient adherence to the oncology treatment regimen:
-
Our primary objective is improving quality of life. We’re not “supposed” to treat the cancer itself, but rather focus more on improving QoL-related symptoms. However, if the patient is receiving immunotherapy…there needs to be an awareness about the side effects…skin-related symptoms need to be seen as a “red flag”, requiring special attention….
Discussion
The three narrative themes identified in this qualitative study highlight the need for a multi-disciplinary approach in the treatment of monoclonal antibody treatment-related dermatological symptoms in the oncology setting. In contrast to the often “fragmented” approach of today’s healthcare, the narrative themes addressed both biophysical and emotional, social, familial, and spiritual aspects of patient care. The first of these themes focused on the biophysical, identifying patient concerns from a comprehensive and systemic perspective shared by HCPs from varied medical disciplines. The second theme addressed the psycho-social domain, recognizing the potential impact of skin lesions on the patient’s body image, sexual and spouse/partner-related concerns, and in which a social, cultural, and spiritual context interacts with the patient’s health-belief model, faith, hope, and ability to cope with uncertainty.
The need for a less fragmented and more holistic perspective regarding dermatological symptoms has become increasingly important during the current COVID-19 pandemic. In the UK, Raza et al. suggested that the shift from face-to-face to virtual outpatient consultations resulting from COVID-19 has been associated with a rise in psychological comorbidities in patients with malignant melanoma, recommending a more holistic approach to patient care. It is their recommendation that clinicians include mental health interventions as part of a “holistic care package” [7]. In the same vein, Julião et al. describe a case of a patient in an end-of-life setting, describing how physical skin complaints, including pain, impacted the patient’s experience within psycho-social, spiritual, and existential domains [8]. Finally, Schuster et al. have made a call for a holistic approach to the treatment of skin disease, with a negative affect and reduced satisfaction with life reported by patients with dermatologic disease, when compared with healthy controls [9].
The third theme identified in the present study addressed the complexity and challenges of a multi-disciplinary setting of care, in which effective communication was believed to ensure integration with continuity of care. The multi-disciplinary approach in dermatology has been reported in a previous study of pediatric patients with epidermolysis bullosa, resulting in improved quality of life-related outcomes and greater adherence to treatment [10]. The multi-disciplinary approach requires a case manager, who may be one of the HCPs described in the present study, including the integrative physician with training and experience in supportive care. The 3 identified themes can be better addressed by asking patients a series of directed questions during their interaction with oncology HCPs, including patients undergoing treatment with monoclonal antibody drugs (Table 2).
The present study has a number of methodological limitations which need to be addressed in future research. These include the pragmatic nature of the prospective database, which may have created a referral bias among patients referred to the IP consultation and IO treatment program. In addition, the qualitative assessment of narratives from the panel of 6 HCPs, examining a select case series of patients, may not reflect the cohort as a whole.
In conclusion, a multi-disciplinary approach should be considered in order to provide personalized care to oncology patients with dermatological symptoms resulting from treatment with monoclonal antibody drugs. The present study did not examine the effectiveness of the IO model of care. However, the findings of the qualitative analysis of the panel HCP narratives suggest that integrative oncology practitioners may serve as one of the case managers responsible for co-designing a supportive care model for patients suffering from dermatological toxicities of these drugs. However, the role of the integrative physician as a case manager in supportive care needs to be studied further and in depth.
References
Sibaud V (2018) Dermatologic reactions to immune checkpoint inhibitors : skin toxicities and immunotherapy. Am J Clin Dermatol. 19(3):345–361. https://doi.org/10.1007/s40257-017-0336-3
Romito F, Giuliani F, Cormio C, Tulipani C, Mattioli V, Colucci G (2010) Psychological effects of cetuximab-induced cutaneous rash in advanced colorectal cancer patients. Support Care Cancer. 18(3):329–334. https://doi.org/10.1007/s00520-009-0656-9 Epub 2009 May 31
Witt CM, Balneaves LG, Cardoso MJ, Cohen L, Greenlee H, Johnstone P, Kücük Ö, Mailman J, Mao JJ (2017) A Comprehensive definition for integrative oncology. J Natl Cancer Inst Monogr. 2017(52):3–8. https://doi.org/10.1093/jncimonographs/lgx012
Greenlee H, DuPont-Reyes MJ, Balneaves LG, Carlson LE, Cohen MR, Deng G, Johnson JA, Mumber M, Seely D, Zick SM, Boyce LM, Tripathy D (2017) Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J Clin. 67(3):194–232. https://doi.org/10.3322/caac.21397 Epub 2017 Apr 24. PMID: 28436999; PMCID: PMC5892208
Ben-Arye E, Schiff E, Shapira C, Frenkel M, Shalom T, Steiner M (2012) Modeling an integrative oncology program within a community-centered oncology service in Israel. Patient Educ Couns. 89(3):423–429. https://doi.org/10.1016/j.pec.2012.02.011 Epub 2012 Mar 7
Hsieh HF, Shannon SE (2005) Three approaches to qualitative content analysis. Qual Health Res. 15(9):1277–1288. https://doi.org/10.1177/1049732305276687
Raza SA, Cannon D, Nuttall G, Ali FR (2022) Exploring the implications of the first COVID-19 lockdown on patients with melanoma: a national survey. Clin Exp Dermatol. 47(1):114–116. https://doi.org/10.1111/ced.14840 Epub 2021 Sep 8. PMID: 34236708; PMCID: PMC8444712
Julião M, Calçada P, Macias VC, Mendes-Bastos P (2021) Beyond striae cutis: a case report on how physical skin complaints unveiled end-of-life total experience. Palliat Support Care. 19(1):119–121. https://doi.org/10.1017/S1478951520000693
Schuster B, Ziehfreund S, Albrecht H, Spinner CD, Biedermann T, Peifer C, Zink A (2020) Happiness in dermatology: a holistic evaluation of the mental burden of skin diseases. J Eur Acad Dermatol Venereol. 34(6):1331–1339. https://doi.org/10.1111/jdv.16146 Epub 2020 Jan 19
Retrosi C, Diociaiuti A, De Ranieri C, Corbeddu M, Carnevale C, Giancristoforo S, Marchili MR, Salvatori G, Atti MLCD, El Hachem M, Raponi M (2022) Multidisciplinary care for patients with epidermolysis bullosa from birth to adolescence: experience of one Italian reference center. Ital J Pediatr. 48(1):58. https://doi.org/10.1186/s13052-022-01252-3 PMID: 35414096; PMCID: PMC9006505
Acknowledgements
We are grateful to Dr Mordechai Alperin, Head of the Department of Family Medicine, Clalit Health Services Haifa and Western Galilee district, for giving us the opportunity to explore new paths. We acknowledge the contribution of Dr. Michael Ziv, Director of the Department of Dermatology, Emek Medical Center, Afula, Israel, for his help in designing the study methodology.
Author information
Authors and Affiliations
Contributions
EBA and DK organized the trial and collected the data analyzed this study. EBA, DK, and YK planned the study. EBA, DK, YK, and NS carried out the analysis and wrote a draft manuscript. All authors participated in the revision of the manuscript.
Corresponding author
Ethics declarations
Ethical approval
The Ethics Review Board (Helsinki Committee) at the Carmel Medical Center in Haifa, Israel, approved the study protocol, which was registered at ClinicalTrials.gov (NCT01860365).
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kruger, D., Samuels, N., Lacey, J. et al. Exploring a multi-disciplinary model of supportive cancer care for monoclonal antibody treatment-related dermatological symptoms. Support Care Cancer 31, 185 (2023). https://doi.org/10.1007/s00520-023-07642-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00520-023-07642-5