
Abstract
Purpose
Aerobic exercise prescriptions in clinical populations commonly involve target intensities based on cardiopulmonary exercise tests (CPET). CPETs are often discontinued prior to a patient achieving true maximum oxygen consumption (VO2 max) which can adversely affect exercise dose and efficacy monitoring; however, reasons for early discontinuation are poorly reported. Accordingly, we explored the CPET termination reasons in persons with cancer participating in exercise intervention studies.
Methods
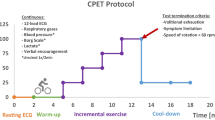
This study comprised of an exploratory, descriptive analysis of retrospective CPET data (VO2 and anaerobic threshold) and termination reasons in a convenience sample of people with cancer participating in exercise intervention studies in a single laboratory. CPETs were standardized using the modified Bruce treadmill protocol with expired gas collection and analysis using a metabolic cart. VO2 max was considered “met” when participants demonstrated (a) oxygen consumption plateau or (b) two of the following criteria: rating of perceived exertion ≥ 9/10, respiratory exchange ratio ≥ 1.15, and/or heart rate of 95% of age-predicted maximum. The frequency and distribution of reasons for test termination relative to the number of CPET exposures for the participants were reported.
Results
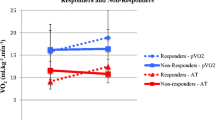
Forty-four participants engaged in exercise studies between February 2016 and March 2018 provided data for the analysis. Participants completed up to three CPETs during this period (total of 78 CPETs in the current analysis). Eighty-six percent of all CPETs were terminated prior to achieving VO2 max verification criteria and no tests resulted in an oxygen consumption plateau. For those that did not demonstrate achievement of VO2 max verification criteria, reasons for discontinuation were distributed as follows: equipment discomfort—49%, volitional peak—36%, and physical discomfort—14.9%. For those who met VO2 max criteria, volitional peak was the most common reason for test termination (45.5%), followed by physical discomfort (36.4%), and equipment discomfort (18.2%).
Conclusions
In our sample of cancer survivors, VO2 max criteria were infrequently met with equipment discomfort being a primary reason for participant-driven test termination. Protocol and equipment considerations are necessary for interpretation and application of CPET findings in clinical practice.

Similar content being viewed by others

Abbreviations
- AT:
-
Anaerobic threshold
- CPET:
-
Cardiopulmonary exercise test
- RER:
-
Respiratory exchange ratio
- QEP:
-
Qualified exercise professional
- ATS/AACP:
-
American Thoracic Society and the American College of Chest Physicians
- HR:
-
Heart rate
- RPE:
-
Rating of perceived exertion
References
Pedersen BK, Saltin B (2015) Exercise as medicine - evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports 25:1–72. https://doi.org/10.1111/sms.12581
Booth FW, Roberts CK, Laye MJ (2012) Lack of exercise is a major cause of chronic diseases. Compr Physiol 2:1143–1211. https://doi.org/10.1002/cphy.c110025.Lack
Schmitz KH, Courneya KS, Matthews C, Demark-Wahnefried W, Galvão DA, Pinto BM, Irwin ML, Wolin KY, Segal RJ, Lucia A, Schneider CM, von Gruenigen V, Schwartz AL, American College of Sports Medicine (2010) American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc 42:1409–1426. https://doi.org/10.1249/MSS.0b013e3181e0c112
Segal R, Zwaal C, Green E, Tomasone JR, Loblaw A, Petrella T, Exercise for People with Cancer Guideline Development Group (2017) Exercise for people with cancer: a clinical practice guideline. Curr Oncol 24:40–46. https://doi.org/10.3747/co.24.3376
Edvardsen E, Hem E, Anderssen SA (2014) End criteria for reaching maximal oxygen uptake must be strict and adjusted to sex and age: a cross-sectional study. PLoS ONE 9:e85276. https://doi.org/10.1371/journal.pone.0085276
Jones LW, Eves ND, Haykowsky M, Joy AA, Douglas PS (2008) Cardiorespiratory exercise testing in clinical oncology research: systematic review and practice recommendations. Lancet Oncol 9:757–765. https://doi.org/10.1016/S1470-2045(08)70195-5
Poole DC, Jones AM (2017) Measurement of the maximum oxygen uptake V̇O2max: V̇O2peak is no longer acceptable. J Appl Physiol 122:997–1002. https://doi.org/10.1152/japplphysiol.01063.2016
Taylor HL, Buskirk E, Henschel A (1955) Maximal oxygen intake as an objective measure of cardio-respiratory performance. J Appl Physiol 8:73–80. https://doi.org/10.1152/jappl.1955.8.1.73
American Thoracic Society, American College of Chest Physicians (2003) ATS/ACCP Statement on Cardiopulmonary Exercise Testing. Am J Respir Crit Care Med 167:211–277. https://doi.org/10.1164/rccm.167.2.211
Aspenes ST, Nilsen TIL, Skaug E-A, Bertheussen GF, Ellingsen Ø, Vatten L, Wisløff U (2011) Peak oxygen uptake and cardiovascular risk factors in 4631 healthy women and men. Med Sci Sports Exerc 43:1465–1473. https://doi.org/10.1249/MSS.0b013e31820ca81c
Niederer D, Vogt L, Gonzalez-Rivera J, Schmidt K, Banzer W (2015) Heart rate recovery and aerobic endurance capacity in cancer survivors: interdependence and exercise-induced improvements. Support Care Cancer 23:3513–3520. https://doi.org/10.1007/s00520-015-2719-4
American College of Sports Medicine (2014) ACSM’s Guidelines for Exercise Testing and Prescription, 9th edn. Lippincott Williams and Wilkins, Baltimore
Wagner DR, Clark NW (2016) Similar results for face mask versus mouthpiece during incremental exercise to exhaustion. J Sports Sci 34:852–855. https://doi.org/10.1080/02640414.2015.1075058
Jones LW, Eves ND, Mackey JR et al (2007) Safety and feasibility of cardiopulmonary exercise testing in patients with advanced cancer. Lung Cancer 55:225–232. https://doi.org/10.1016/j.lungcan.2006.10.006
Bart BA, Wolfel EE (1994) Method of expired gas collection during cardiopulmonary exercise testing does not affect respiratory gas exchange measurements in patients with heart failure. J Card Fail 1:91–96. https://doi.org/10.1016/1071-9164(94)90012-4
Neuberg GW, Friedman SH, Weiss MB, Herman MV (1988) Cardiopulmonary exercise testing. The clinical value of gas exchange data. Arch Intern Med 148:2221–2226
Forman DE, Myers J, Lavie CJ, Guazzi M, Celli B, Arena R (2010) Cardiopulmonary exercise testing: relevant but underused. Postgrad Med 122:68–86. https://doi.org/10.3810/pgm.2010.11.2225
Milani RV, Lavie CJ, Mehra MR, Ventura HO (2006) Understanding the basics of cardiopulmonary exercise testing. Mayo Clin Proc 81:1603–1611. https://doi.org/10.4065/81.12.1603
Segal R, Zwaal C, Green E, Tomasone JR, Loblaw A, Petrella T, Exercise for People with Cancer Guideline Development Group (2017) Exercise for people with cancer: a systematic review. Curr Oncol 24:e290–e315. https://doi.org/10.3747/co.24.3619
Steins Bisschop CN, Velthuis MJ, Wittink H, Kuiper K, Takken T, van der Meulen W, Lindeman E, Peeters PH, May AM (2012) Cardiopulmonary exercise testing in cancer rehabilitation. Sports Med 42:367–379. https://doi.org/10.2165/11598480-000000000-00000
Kenjale AA, Hornsby WE, Crowgey T, Thomas S, Herndon JE 2nd, Khouri MG, Lane AR, Bishop CE, Eves ND, Peppercorn J, Douglas PS, Jones LW (2014) Pre-exercise participation cardiovascular screening in a heterogeneous cohort of adult cancer patients. Oncologist 19:999–1005. https://doi.org/10.1634/theoncologist.2014-0078
Scharhag-Rosenberger F, Wiskemann J, Scharhag J (2015) Cardiopulmonary exercise testing in cancer patients: should we really refrain from considering it for preparticipation screening? Oncologist 20:228–228. https://doi.org/10.1634/theoncologist.2014-0366
Lerman J, Bruce RA, Sivarajan E, Pettet GE, Trimble S (1976) Low-level dynamic exercises for earlier cardiac rehabilitation: aerobic and hemodynamic responses. Arch Phys Med Rehabil 57:355–360
Beaver WL, Wasserman K, Whipp BJ (1986) A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol (Bethesda, Md : 1985) 60:2020–2027. https://doi.org/10.1152/jappl.1986.60.6.2020
Elborn JS, Stanford CF, Nicholls DP (1990) Reproducibility of cardiopulmonary parameters during exercise in patients with chronic cardiac failure. The need for a preliminary test. Eur Heart J 11:75–81. https://doi.org/10.1093/oxfordjournals.eurheartj.a059596
Barron A, Dhutia N, Mayet J, Hughes AD, Francis DP, Wensel R (2014) Test-retest repeatability of cardiopulmonary exercise test variables in patients with cardiac or respiratory disease. Eur J Prev Cardiol 21:445–453. https://doi.org/10.1177/2047487313518474
Wasserman K (1986) The anaerobic threshold: definition, physiological significance and identification. Adv Cardiol 35:1–23
DZH L, Jack S, Swart M, Carlisle J, Wilson J, Snowden C, Riley M, Danjoux G, Ward SA, Older P, MPW G, Perioperative Exercise Testing and Training Society (POETTS) (2018) Perioperative cardiopulmonary exercise testing (CPET): consensus clinical guidelines on indications, organization, conduct, and physiological interpretation. Br J Anaesth 120:484–500. https://doi.org/10.1016/j.bja.2017.10.020
Sullivan MJ, Cobb FR (1990) The anaerobic threshold in chronic heart failure. Relation to blood lactate, ventilatory basis, reproducibility, and response to exercise training. Circulation 81:II47–II58
Meyer T, Gorge G, Schwaab B et al (2005) An alternative approach for exercise prescription and efficacy testing in patients with chronic heart failure: a randomized controlled training study. Am Heart J 149:e1-7. https://doi.org/10.1016/j.ahj.2004.12.006
Zatloukal B, Toman J, Homolka P et al (1995) Anaerobic threshold determination and its importance in chronic heart failure patients. Sports Med Train Rehabil 5:255–272. https://doi.org/10.1080/15438629509512023
Lee CHA, Kong JC, Ismail H et al (2018) Systematic review and meta-analysis of objective assessment of physical fitness in patients undergoing colorectal cancer surgery. Dis Colon Rectum 61:1. https://doi.org/10.1097/DCR.0000000000001017
Tsai H-Y, Tsai W-J, Kuo L-Y et al (2018) Oxygen consumption at anaerobic threshold predicts cardiac events after heart transplantation. Transplant Proc. https://doi.org/10.1016/j.transproceed.2018.03.096
Older P, Smith R, Courtney P, Hone R (1993) Preoperative evaluation of cardiac failure and ischemia in elderly patients by cardiopulmonary exercise testing. Chest 104:701–704. https://doi.org/10.1378/chest.104.3.701
Dunne DFJ, Jack S, Jones RP, Jones L, Lythgoe DT, Malik HZ, Poston GJ, Palmer DH, Fenwick SW (2016) Randomized clinical trial of prehabilitation before planned liver resection. Br J Surg 103:504–512. https://doi.org/10.1002/bjs.10096
Berkel AEM, Bongers BC, van Kamp M-JS et al (2018) The effects of prehabilitation versus usual care to reduce postoperative complications in high-risk patients with colorectal cancer or dysplasia scheduled for elective colorectal resection: study protocol of a randomized controlled trial. BMC Gastroenterol 18:29. https://doi.org/10.1186/s12876-018-0754-6
Gitt AK, Wasserman K, Kilkowski C, Kleemann T, Kilkowski A, Bangert M, Schneider S, Schwarz A, Senges J (2002) Exercise anaerobic threshold and ventilatory efficiency identify heart failure patients for high risk of early death. Circulation 106:3079–3084
Opasich C, Pinna GD, Bobbio M, Sisti M, Demichelis B, Febo O, Forni G, Riccardi R, Riccardi PG, Capomolla S, Cobelli F, Tavazzi L (1998) Peak exercise oxygen consumption in chronic heart failure: toward efficient use in the individual patient. J Am Coll Cardiol 31:766–775. https://doi.org/10.1016/S0735-1097(98)00002-3
Albouaini K, Egred M, Alahmar A, Wright DJ (2007) Cardiopulmonary exercise testing and its application. Postgrad Med J 83:675–682
Mann T, Lamberts RP, Lambert MI (2013) Methods of prescribing relative exercise intensity: physiological and practical considerations. Sports Med 43:613–625. https://doi.org/10.1007/s40279-013-0045-x
West MA, Astin R, Moyses HE, Cave J, White D, Levett DZH, Bates A, Brown G, Grocott MPW, Jack S (2019) Exercise prehabilitation may lead to augmented tumor regression following neoadjuvant chemoradiotherapy in locally advanced rectal cancer. Acta Oncol 58:588–595. https://doi.org/10.1080/0284186X.2019.1566775
Dimeo F, Schwartz S, Wesel N et al (2008) Effects of an endurance and resistance exercise program on persistent cancer-related fatigue after treatment. Ann Oncol 19:1495–1499. https://doi.org/10.1093/annonc/mdn068
Ewer MS, Ewer SM, Suter T (2017) Cardiac complications of cancer treatment. In: Bast RC Jr, Croce CM, Hait WN et al (eds) Holland-Frei Cancer Medicine, 9th edn. Wiley, Hoboken, pp 1763–1780
Brubaker PH, Kitzman DW (2011) Chronotropic incompetence: causes, consequences, and management. Circulation 123:1010–1020. https://doi.org/10.1161/CIRCULATIONAHA.110.940577
Hughes DC, Cox MG, Serice S, Baum G, Harrison C, Basen-Engquist K (2017) Using rating of perceived exertion in assessing cardiorespiratory fitness in endometrial cancer survivors. Physiother Theory Pract 33:758–765. https://doi.org/10.1080/09593985.2017.1357150
Schmidt K, Vogt L, Thiel C, Jäger E, Banzer W (2013) Validity of the six-minute walk test in cancer patients. Int J Sports Med 34:631–636. https://doi.org/10.1055/s-0032-1323746
Cohen-Solal A, Beauvais F, Tabet JY (2007) Cardiopulmonary exercise testing in chronic heart failure. In: Perk J, Mathes P, Gohlke H et al (eds) Cardiovascular Prevention and Rehabilitation, 1st edn. Springer London, London, pp 99–109
Farley RS, Ray PS, Moynihan GP (1998) Evaluation of three gas collection devices. Int J Ind Ergon 22:431–437. https://doi.org/10.1016/S0169-8141(97)00013-9
Boulé NG, Robert C, Bell GJ, Johnson ST, Bell RC, Lewanczuk RZ, Gabr RQ, Brocks DR (2011) Metformin and exercise in type 2 diabetes: examining treatment modality interactions. Diabetes Care 34:1469–1474. https://doi.org/10.2337/dc10-2207
Hoogeveen A, Schep G, Hoogsteen J (1999) The Ventilatory threshold, heart rate, and endurance performance: relationships in elite cyclists. Int J Sports Med 20:114–117. https://doi.org/10.1055/s-2007-971103
James DVB, Doust JH (1998) Oxygen uptake during moderate intensity running: response following a single bout of interval training. Eur J Appl Physiol 77:551–555. https://doi.org/10.1007/s004210050375
Acknowledgments
We would like to acknowledge Alyssa Franzese, Kailey Trewartha, and Manesha Khazanchi for their assistance in participant data collection and entry.
Funding
The studies of participants included in this analysis were funded by the Canadian Breast Cancer Foundation and the Princess Margaret Cancer Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This analysis was approved by the University Health Network Research Ethics Board and all participants provided written informed consent for their respective studies.
Conflict of Interest
The authors declare that they have no conflict of interest.
Disclaimer
The authors have full control of all primary data and datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Santa Mina, D., Au, D., Papadopoulos, E. et al. Aerobic capacity attainment and reasons for cardiopulmonary exercise test termination in people with cancer: a descriptive, retrospective analysis from a single laboratory. Support Care Cancer 28, 4285–4294 (2020). https://doi.org/10.1007/s00520-019-05094-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-019-05094-4