
Abstract
Recent insights in allorecognition and graft rejection mechanisms revealed a more complex picture than originally considered, involving multiple pathways of both adaptive and innate immune response, supplied by efficient inflammatory synergies. Current pillars of transplant monitoring are serum creatinine, proteinuria, and drug blood levels, which are considered as traditional markers, due to consolidated experience, low cost, and widespread availability. The most diffuse immunological biomarkers are donor-specific antibodies, which are included in routine post-transplant monitoring in many centers, although with some reproducibility issues and interpretation difficulties. Confirmed abnormalities in these traditional biomarkers raise the suspicion for rejection and guide the indication for graft biopsy, which is still considered the gold standard for rejection monitoring. Rapidly evolving new “omic” technologies have led to the identification of several novel biomarkers, which may change the landscape of transplant monitoring should their potential be confirmed. Among them, urinary chemokines and measurement of cell-free DNA of donor origin are perhaps the most promising. However, at the moment, these approaches remain highly expensive and cost-prohibitive in most settings, with limited clinical applicability; approachable costs upon technology investments would speed their integration. In addition, transcriptomics, metabolomics, proteomics, and the study of blood and urinary extracellular vesicles have the potential for early identification of subclinical rejection with high sensitivity and specificity, good reproducibility, and for gaining predictive value in an affordable cost setting. In the near future, information derived from these new biomarkers is expected to integrate traditional tools in routine use, allowing identification of rejection prior to clinical manifestations and timely therapeutic intervention. This review will discuss traditional, novel, and invasive and non-invasive biomarkers, underlining their strengths, limitations, and present or future applications in children.
Similar content being viewed by others



Introduction
The current view of allorecognition and graft rejection mechanisms is that of a highly complex and articulated phenomenon, where inflammatory processes synergize with adaptive immune responses resulting in T or B cell activation. This complexity is incompletely captured by the traditional laboratory tools used for monitoring graft health, and therefore, rejection monitoring remains an unmet clinical need.
Current pillars of transplant monitoring include traditional markers, such as serum creatinine, proteinuria, and drug blood levels, implemented by immunological biomarkers such as donor specific antibodies (DSA) [1]. Perturbations of these biomarkers guide the indication for graft biopsy, which is still considered the gold standard for rejection diagnosis.
The limits of these markers and the invasiveness of repeated biopsies, particularly in children, could be overcome by integration with the information provided by rapidly evolving novel biomarkers, which are currently used in limited clinical settings, particularly in children [2].
In the pediatric setting, overall results of kidney transplantation remain unsatisfactory in the long run, in particular when passing through the risky years of adolescence. A recent study highlighted the excess of late acute rejection episodes in the NAPRTCS cohort [3], pointing out the need to increase the performances of surveillance modalities after the generally adopted schedules of intensive monitoring of the first 24 months.
The ideal biomarker
The basic definition of a biomarker is that of a defined characteristic, objectively measured and evaluated as an indicator of normal or pathogenic biological processes or responses to an exposure or intervention, which can be derived from molecular, histologic, radiographic, or physiologic characteristics.
A number of biomarkers can be identified with diagnostic, monitoring, response, predictive, prognostic, safety, and susceptibility/risk values. The NIH-FDA Biomarker Working Group has recently defined the characteristics of an ideal biomarker in the BEST Resource. (Details and reference are in Supplementary Table 1.)
One of the main characteristics of a biomarker is the capability to identify patients with high disease probability, avoiding false over/under-rating of different independent cohorts. The diagnostic/predictive accuracy of a biomarker is therefore very important to allow its confident use and is generally expressed by specific metrics data: sensitivity and specificity and the related area under the receiver operator characteristic curve (see Supplementary Table 1).
The predictive value of the biomarker is the capacity to predict a clinically relevant event: the negative predictive value (NPV) allows excluding confidently the disease, while the positive predictive value (PPV) confirms the disease status. A monitoring and predictive biomarker should change significantly in response to treatment, while a prognostic biomarker should predict a clinical outcome regardless of treatment, meaning that it can be used to determine the risk of a bad prognosis.
Laboratory tests considering biomarkers should possess a number of requirements, including characteristics of robust reproducibility and interpretability, as well as external validation confirming good performance metrics.
One further step is the use of a biomarker as a surrogate end point, as a tool for early detection of a certain condition. In the field of transplantation, a certain value could be considered a surrogate end point of rejection and be the threshold to proceed with biopsy or directly to treatment [4].
Traditional biomarkers in transplantation and their limitations
Creatinine is the most commonly employed measurement to determine kidney function. While widely available and cheap, it is neither specific nor sensitive and is often a late indicator of subclinical rejection. This is particularly true in children receiving large grafts, as demonstrated by the frequent finding of subclinical histological rejection evident in protocol biopsies, with no modification in serum creatinine [5].
Among other kidney function tests, proteinuria is routinely measured and is considered as being among the standard of care. Its performance as a biomarker for rejection is, however, low, in children: albuminuria and proteinuria are nonspecific signs of allograft injury with high sensitivity for graft loss but low specificity. In the large adult cohort described in [6], early detection of proteinuria > 1 g/24 h displayed low sensitivity and high specificity for graft loss at 5 years (AUC 0.64, sensitivity 0.10; specificity 0.95), with increasing accuracy over time (AUC 0.71, 0.73, and 0.77, respectively, at 1, 3, and 5 years) but still low sensitivity (from 0.16 at 1 year to 0.28 at 5 years) and good specificity (from 0.95 at 1 year to 0.96 at 5 years). Proteinuria had a negative predictive value (91–93%) at any time, but no specific analysis considered the full T cell–mediated rejection/antibody-mediated rejection (TCMR/ABMR) definition. No specific prospective studies have explored the performance of the protein/creatinine ratio as a biomarker for rejection in children.
Surveillance protocol biopsy
At present, tissue biopsy remains the gold standard for assaying the health of the graft, although arguments on specificity and sensitivity of histology lesions and their predictive value, particularly when performed early after transplant, are reported in different studies. Protocol surveillance biopsies possess the advantage of an unbiased longitudinal approach, but represent invasive procedures, particularly in small children: are risky mainly for occurrence of adverse events, such as bleeding and artero-venous fistula, time-consuming, subject to pathology interpretation, and generally limited to the first 12–24 months after transplantation. The role of protocol biopsies as modifiers of long-term allograft survival in children remains debated, due to different induction and maintenance immunosuppressive regimens, timing of biopsy, and policy for management of subclinical rejection [2, 4, 7]. At the same time, the incidental finding of non-specific signs of chronic allograft damage without actionable inflammation is a problematic issue even in per cause biopsies. Subclinical TCMR signs are reported in a significant unexpected proportion of patients in several retrospective series [2], reinforcing the advantages of preemptive treatment on longer graft survival [8]. On the other side, in a recent prospective trial, children with stable serum creatinine at 6 months and Banff lesions from borderline to Ia, Ib, or IIa were not treated and GFR remained stable at 24 months, independently of biopsy findings, suggesting that surveillance biopsy at 6 months could be spaced out in stable low-risk patients [4].
A recent survey in adult centers in the USA [9] reported that surveillance biopsy policy is adopted in 46% of the centers, underlying the notion that noninvasive immunological monitoring is perceived as unsatisfactory. However, the notion of repeated histology monitoring remains controversial, arguing for the need for controlled studies.
In the Canadian PROBE multicenter study [10], adjunctive control post-treatment biopsies were generally performed after a diagnosis of rejection during surveillance biopsies, frequently highlighting persistent inflammation. These findings raise concerns that the common use of functional monitoring to adjudicate rejection resolution is likely insufficient and not sensitive enough to confidently consider the rejection episode properly treated and solved.
Altogether, these reasons argue for the need to find additional noninvasive or minimally invasive monitoring systems that can be performed easily, diffusely, and longitudinally over time to continuously patrol subclinical rejection, evaluate evolution of the immunological phenomena upon treatment, and to allow personalized optimization of therapy until a successful resolution is confidently reached.
Drug level monitoring
Drug level monitoring is generally accepted as a biomarker of proper immunosuppressive drug use. It is routinely performed for tacrolimus, cyclosporin, everolimus, and sirolimus. Mycophenolic acid single sample trough concentration is not a good surrogate for overall exposure of the drug. These limits are overcome by mycophenolic acid area under the curve (AUC) estimation, which proved to be an effective tool, although less practical, particularly in children, due to the need for at least 2 or 3 concentration samplings for mycophenolate mofetil and 3 to 4 samplings for mycophenolic acid assay [11]. Steroid effective dose determinations are still lacking.
Fluctuations in tacrolimus blood levels in individual patients at a fixed dose over time are defined as intra-patient variability (IPV). High tacrolimus IPV in adult studies correlates with development of DSA, allograft dysfunction, rejection, transplant glomerulopathy, and late graft loss (reviewed in Kuypers) [12].
In the few pediatric studies, tac IPV correlates with de novo DSA development. However, in children, the correlation with rejection, function decline, and graft loss is weaker likely due to biases in defining cut-off values, cohort numerosity, and methodological differences [13, 14] (detailed in Supplementary Table 2).
Future perspectives should advocate expert systems to estimate drug exposure [15], novel techniques to evaluate multiple drugs simultaneously, and the transition to the concept of “time in therapeutic range”, already adopted in other fields, as more precise predictors of under-suppression and potential risk of allograft rejection [16].
Donor-specific antibodies
Donor-specific antibodies (DSA) are antibodies developed by the transplant recipient against specific HLA antigens present on the donor kidney. Rejection mediated by DSA may be acute if the graft is exposed to rapid increases in high-titer DSA, which may be generated in sensitized recipients or which may represent de novo responses in non-sensitized patients who are non-adherent to immunosuppressive therapy. On the other hand, chronic rejection mediated by DSA is associated with a slower appearance of antibodies, which may be high or low titer and transient or persistent [17].
These antibodies may damage the kidney by causing multi-lamination of the peritubular capillary basement membrane or arteriopathy manifesting as intimal fibrosis [17]. It is well established that the development of de novo DSA (dnDSA) after kidney transplantation is linked to poor graft outcomes in both adults and children [18, 19]. The effects of the sequelae of chronic antibody-mediated rejection are more difficult to control.
For these reasons, dnDSA represent an established biomarker predictive of late acute antibody-mediated rejection, chronic antibody-mediated rejection, transplant glomerulopathy, and graft loss [1], demonstrated also in children [19, 20].
Some firm points concerning the role of DSA in chronic allograft damage can be made:
-
1.
DSA can be detected in the serum of kidney transplant recipients years prior to clinical graft dysfunction. For these reasons, it is important to monitor DSA routinely in the follow-up of transplant recipients, even though homogeneous protocols are lacking [19].
-
2.
The clinical relevance of dnDSA relies on characteristics of the antibody itself, such as the IgG subclass, influencing the capability to bind complement and recruit effector cells through Fc receptor binding. DSA of IgG3 subclass bind C1q more efficiently, activate the classical pathway of complement cascade, and proceed more frequently to acute antibody-mediated rejection, while DSAs of IgG4 subclass are unable to bind complement and act mainly through the Fc receptor to amplify alloresponses [21].
-
3.
In general, dnDSA formation has been associated with lower 10‐year graft survival, including in pediatric studies [19].
-
4.
DSAs are generally measured by the single antigen Luminex technology, where the mean fluorescence intensity (MFI) is a proxy of the intensity of binding of the antibody contained in the patient serum to the beads. Consistently, higher MFI levels have been associated with impaired graft function, even though exceptions occur [22].
-
5.
While there is intense investigation around therapeutic strategies aimed at reducing DSA levels [23], little is known about how to prevent initial DSA formation. Likewise, determination of risk factors for DSA development has not been fully characterized. Preliminary evidence suggests that the type of immunosuppressive therapy may impact DSA development [24]. Specifically, regimens based on calcineurin inhibitors appear less likely to be associated with DSA formation, compared to regimens based on mTOR inhibitors or lower mycophenolic acid levels [25] (Fig. 1).
Fig. 1 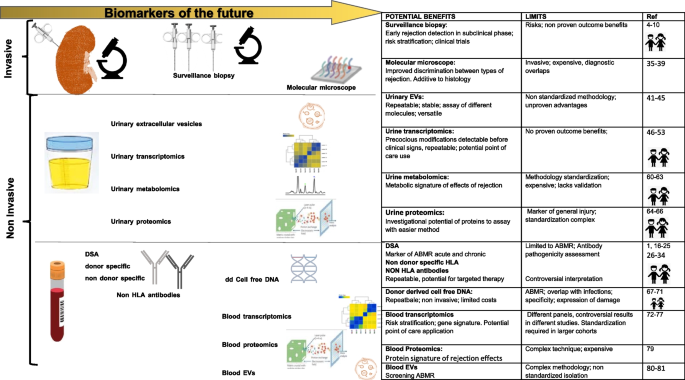
Traditional and novel biomarkers for kidney rejection diagnosis. Invasive and non-invasive biomarkers obtained from urine and from blood evaluated in children and adults at the present time, with benefits and limitations

Non-donor-specific anti-HLA antibodies
The finding of non-donor-specific antibodies (NDSA), i.e., antibodies which are directed against HLA specificities other than the donor mismatched antigens, is a relatively common finding in post-transplant monitoring. While pre-transplant NDSAs have been demonstrated to have a detrimental role in graft outcome, the clinical significance of de novo NDSA (dnNDSA) is much more controversial [26]. Some studies have showed that post-transplant occurrence of dnNDSA in non-sensitized kidney graft recipients does not have an adverse effect on graft survival [19, 27], while others evidenced that patients developing dnNDSA have an increased risk of graft failure [28,29,30]. However, in all instances, patient cohorts have a short to medium post-transplant follow-up, with NDSA usually analyzed at a single time point [26], somewhat limiting the impact of these observations and arguing in favor of more structured studies (Fig. 1).
Non-HLA antibodies
The observation that a significant subset of patients with histological features of antibody-mediated rejection (AMR) in the graft biopsy lacks evidence of dnDSA [31] was the starting point in the identification of non-HLA DSA [32].
Although the first reports connecting non-HLA antibodies and graft outcome were published in 2005 [33], their actual role in rejection remains debated. Among the different targets identified are antibodies against specific alloantigens such as MHC class I chain-related gene A (MICA-Ab) or B (MICB), or against autoantigens like endothelin-1 type A receptor (ETAR-Ab), perlecan, agrin, or vimentin, among others. Antibodies against angiotensin II type 1 receptor (AT1R-Ab) are among the most studied, including in pediatric patients [34] (Fig. 1).
Biomarkers of the future (Table 1 and Fig. 1)
Innovative diagnostics on tissue biopsies
“Tissue transcriptomics” relies upon analysis of mRNA transcripts on biopsy tissue fragments on a microarray technology. This technology provides a complementary quantitative and reproducible tool for deeper and more accurate graft biopsy analysis.
The microarray-based molecular diagnostic system MMDX®, known as “molecular microscope,” was set on an initial discovery study on 403 biopsies, and validated on a further independent cohort of 300 biopsies. The study identified a universal set of mRNA changes and specific sets of mRNA transcripts for TCMR and ABMR [35, 36]. Prominent transcripts of both rejections were interferon-γ (IFN-γ)-inducible genes in several types of cells. Based on these findings, different pathways were defined for TCMR-specific transcripts, including effector T cells, such as CTLA4, ICOS, and costimulatory molecules, macrophage infiltration, and activation molecules, such as IFN-γ-inducible CD80, CD86, and ANKRD22. ABMR selective transcripts, such as CCL4, CXCL11, and CXCL9 resulted expressed only in NK cells or in endothelial cells. Some other markers proved specific for advanced phases of ABMR. Despite some overlap between the types of rejection, the association of transcripts with the subtypes of rejection is quite strong, as demonstrated by the multicenter INTERCOM study [37], which allowed the identification of ABMR in a high percentage of C4d and histology negative biopsies.
Another commercially available platform is the Nanostring® B-HOT panel, set up by the Banff Working Group in 2019, including 770 genes, pertinent to rejection, tolerance, viral infections, innate and adaptive immune responses, categorized on functional annotations for different pathways [38].
Based on the same technology, the GoCAR study defined a gene set capable of predicting kidney allografts at risk of progressive injury due to fibrosis [39]. In this study, the authors identified a set of 13 genes which proved independently predictive for the development of fibrosis at 1 year, superior to clinical and histology variables. The predictive value of this gene set was validated in an independent cohort from the GoCAR study and two independent, publicly available expression datasets (Fig. 1).
Non-invasive novel urinary biomarkers
Urine matrix represents an appealing substrate for the development of a rejection biomarker, being the direct ultrafiltrate where, at least theoretically, an early perturbation of the usual asset can be assessed noninvasively. Some innovative methodological approaches adopted extracellular vesicle focused studies, assaying the lipid, protein, or mRNA content or combined transcript analysis with ELISA assay of target proteins.
Moreover, the development of new high-throughput techniques allowing the use of multiple”omics” assays rapidly led to different interesting studies evaluating mRNA transcripts, urinary metabolites, protein panels, and genomes in urine (Fig. 1 and Table 1).
Urinary extracellular vesicles
Extracellular vesicles (EVs) are membrane vesicles released by all cell types with the capacity of transmitting signaling molecules to the surrounding environment and exerting a multitude of paracrine end endocrine effects in physiological and pathological conditions [40]. EVs are lipid bi-layered particles released from plasma membranes and are highly heterogenous for origin, size, and content. They carry proteins, lipids, nucleic acids, or other bioactive molecules specific to the parental cell of origin and are retrieved in plasma and urine in several forms ranging from 30–100 nm (exosomes) to 100–1000 nm (microvesicles) and with different density and protein markers. Accurate characterization in EV research studies is crucial, although still not standardized: the International Society for Extracellular Vesicles recommends size definition, quantification, characterization of surface and cytosolic proteins, and imaging for extracellular vesicle proper description and study comparison. These technical challenges render ample and multicenter clinical studies inevitably difficult.
In the field of transplantation, EVs circulating in plasma and secreted in urine are of high interest for the capacity to carry information originating directly from the grafted kidney or from the host immune system and are considered of enormous potential as non-invasive biomarkers.
Urinary EVs were studied in the setting of acute rejection on a proteomic profile: eleven proteins functionally involved in inflammatory and stress response were identified, with 3 exclusively urinary proteins more abundant in patients with acute rejection [41]. Other proteomic studies identified urinary protein biomarkers associated with acute cellular rejection (ACR), able to discriminate between acute cellular or antibody-mediated rejection and chronic active antibody rejection [42, 43].
Recent approaches focused on the detection of CD3 expressing urinary EVs as carriers of messages originating directly from infiltrating T lymphocytes [44]. Specific mRNA multigene signatures were identified with a good specificity for acute rejection in a series of 192 urine samples collected simultaneously to indication biopsy. The signature revealed mRNA encoding for CXCL11, CD74, IL32, STAT1,CXCL14, SERPINA1, B2M, C3, PYCARD, BMP7, TBP, NAMPT, IFNGR1, IRAK2, and IL18BP [45]. In the same study, the authors identified another multigene signature (CD74, C3, CXCL11, CD44, and IFNAR2) that could distinguish TCMR from ABMR. Since RNA molecules are well protected inside the EVs, they can be assessed from urine samples even after prolonged storage, whereas proteins that are associated with the outer membrane of the EVs are exposed to protease activity and are less stable. mRNA evaluation, therefore, seems to offer the methodological advantages of an applicable biomarker.
The major limitations for a widespread diffusion of these biomarkers at the present time are mainly a lack of standardized procedures in isolation, purification, and characterization, which could potentially be solved by technological investment on commercially available kits. Another issue is the different experimental protocols adopted for assaying nucleic acids or proteins with different methodologies, rendering comparison of single studies and interpretation of results difficult. Moreover, no studies so far have included children (Fig. 1 and Table 1).
Urine transcriptomics
Urine mRNA transcripts were analyzed in several studies using different panels and approaches: in the CTOT-04 study, a set of urinary mRNAs (CD3ε, perforin, granzyme B, proteinase inhibitor 9, CD103, IP-10, CXCR3, transforming growth factor β1 [TGF-β1]) and 18S ribosomal RNA) was prospectively analyzed in 485 patients in the first year post-transplantation. A three-gene signature (CD3ε, interferon-inducible protein 10 (IP-10) formerly known as CXCL10, 18S rRNA) was identified as able to discriminate ACR [46]. Moreover, analysis of the trajectories before the biopsy showing acute rejection demonstrated a marked increase in the three-gene signature starting from 120 days before rejection was clinically apparent. A significant modification in gene expression following adjustments to immunosuppressive protocol was also observed, suggesting that this signature may be useful in monitoring immune status [46]. In a further pilot study, still requiring validation, a 5-gene signature (CD3ε, CD105, CD14, CD46, and 18S rRNA) further distinguished ACR from AMR [47].
Starting from biopsy material originating from different solid organ transplants, a common rejection module was identified and evaluated also in urine, where overexpression of BASP1, CD6, CXCL10, CXCL9, INPP5D, ISG20, LCK, NKG7, PSMB9, RUNX3, and TAP1 was evidenced in the presence of acute rejection [48]. In other studies, such as the CTOT-1, where the previous mentioned panels were studied, the CXCL9 chemokine and the corresponding protein alone were able to provide the best predictive value for diagnosing or excluding acute rejection. In that study, mRNA levels were highly sensitive and were an early marker of rejection, with levels rising at least 30 days before clinical signs [49]. In this context, the CRISPR–Cas13 method combined with the specific high-sensitivity enzymatic reporter unlocking (SHERLOCK) technology for the detection of CXCL9 mRNA in urine is among the most attractive systems [50]. In this study, higher CXCL9 mRNA levels are observed in samples from patients with biopsy-proven rejection compared with transplant recipients with no rejection or stable graft function, with a sensitivity of 93%. Furthermore, the assay, which could detect CLCX9 at the attomolar range, was combined with the lateral flow-based system on a dipstick readable with a smartphone to allow quantification of band intensity. This advanced technique that allows accurate monitoring of CXCL9 mRNA levels represents the most auspicious near future for a valuable biomarker, for its potential easy applicability, outside of transplant centers, where most of the patients are effectively being followed over time. However, the high potential of urinary mRNA assays is hampered by methodological limits due to mRNA degradation in urine, poor sample processing, and storage conditions for centralized analysis. Therefore, technology improvement is urgently needed to allow better standardization.
Other limited studies addressed microRNAs (miRNAs) as urinary biomarkers of rejection. MiRNAs are endogenous, single-stranded molecules of non-coding nucleotides able to repress the expression of target genes through the post-transcriptional degradation of mRNA and inhibition of protein expression. MiRNAs therefore retain an immunomodulant activity in innate and adaptive immune response. Lorenzen et al. studied a panel of 3 deregulated miRNAs and noted that levels of miR-10b and -210 were decreased and miR-10a increased in patients with acute renal allograft rejection. MiR-210 was predictive of GFR decline 1 year after transplantation and was able to differentiate patients with ACR from urinary tract infection [51].
Other miRNAs, including miR-142-3p, miR-210-3p, and miR-155-5p, were reported by Millàn et al. [52] to be deregulated in acute rejection. Among them, miR-155-5p proved to have the highest sensitivity and specificity and good negative and positive predictive values.
More recently, a combined approach of miRNAs [53] and urinary assay of CXCL-9 and CXCL-10 chemokine levels using a multivariable model evidenced that miR-155-5p, miR-615-3p, and CXCL-9 levels were independent predictors of rejection. Levels of miR-155-5p, miR-126-3p, miR-21-5p, miR-25-3p, and miR-615-3p were significantly different between rejection and no-rejection urine; CXCL-9 and CXCL-10 protein levels were significantly elevated in urine from recipients with rejection, and the combination of these biomarkers produced a model with better diagnostic performance than the single biomarkers [53] (Fig. 1 and Table 1).
Urinary chemokines
Chemokines are secreted by leukocytes upon interferon γ stimulation and are critical regulators of leukocyte recruitment during allograft rejection. CXCL10 and CXCL9 upregulation was demonstrated by mRNA expression and protein synthesis increase in urine and blood in different models. Several studies of adults and 4 studies of children proved that urinary chemokines are valuable biomarkers for early detection of subclinical and clinical TCMR and for accurate monitoring of the response to treatment [54,55,56,57].
A recent multicenter, prospective study within the Predicting Renal transplant Outcome using BiomarkErs (PROBE) cohort demonstrated that CXCL10/Cr, assayed in urine paired with protocol biopsy, was significantly increased in rejection and declined upon treatment [58]. More interestingly, CXCL10/Cr rose 3–4 weeks prior to biopsy in cases with rejection, representing a potential tool for serial urinary surveillance and decision-making on biopsy timing and indication. The main limitation of the assay is its inability to distinguish between rejection and BKV infection or urinary infection.
The VIRTUUS prospective pediatric multicenter study is ongoing and aims to validate a urinary mRNA and metabolomics profile as diagnostic and prognostic biomarker of ACR using a urinary cell mRNA 3-gene signature including CXCL10 mRNA [59] (Fig. 1 and Table 1).
Urinary metabolomics
Perturbations of kidney tissue metabolism can be assessed in urine with an unbiased “omic” approach known as “metabolomics”. This mass spectrometry-based method simultaneously measures multiple metabolites. The aim, adopted by independent groups, was to define a distinct and specific metabolic signature for rejection and other kidney diseases.
In a recent study performed in a pediatric kidney transplant cohort [60] including 30 TCMR and 54 borderline tubulitis, ten metabolites, namely proline, kynurenine, sarcosine, methionine sulfoxide, threonine, glutamine, phenylalanine, alanine, and PC.aa.C34.4 and PC.ae.C38.6, produced by activated macrophages and T helper 1 subsets, displayed a good correlation with cellular rejection. The study however has some methodological limitations and needs to be confirmed in other patient cohorts.
The pilot study of Banas et al. [61] defined in NMR-spectroscopy another set of candidate markers, namely, alanine, citrate, dimethylamine (DMA), glucose, glucuronate, hippurate, lactate, phenylacetylglutamine (PAQ), trigonelline, and urea, able to discriminate rejection. Metabolites such as lactate may represent the downstream products of cellular activity and mitochondrial derangement as in tubular damage, and it is of note that no soluble metabolites of clear lymphocyte origin were identified.
The same methodological approach is now being applied in a multicenter cohort comprising 972 histologically and clinically characterized patients in the PARASOL study [62], aiming at validating a metabolic signature of rejection with good predictive value.
Very promising is the employment of combined “omics” such as the QSant assay [63], which integrates the measurement of urinary cell-free DNA, methylated-cell-free DNA, total proteins, CXCL-10, clusterin, and creatinine. By using an artificial intelligence algorithm, results are expressed as a Q score ranging from 0 to 100, which discriminates with a good predictive value between acute rejection and no rejection (Fig. 1 and Table 1).
Urinary proteomics
Urine proteomics, similar to the other “omic” sciences, relies on a large-scale study approach without the bias of a hypothetical selection of urinary proteins. Concerning a complex phenomenon like rejection, the amount of the generated data and the different experimental conditions have produced interesting results to date, but not a generalized consensus toward the choice of the different profiles.
One of the most interesting contributions in children identified by capillary electrophoresis-mass spectrometry (CE-MS) is a urinary proteomic profile of 79 proteins able to distinguish with good performance chronic active ABMR and was validated also in an independent cohort [64, 65]. It is of note that most of the proteins were fragments of collagen, alpha-1-antitrypsin, retinol-binding protein 4, fibrinogen alpha chain, neurosecretory protein VGF, Ig kappa chain C region, beta-2-microglobulin, and annexin A, but that no immunologically active proteins were detected.
Another recent study [66] described a panel of the ten most-represented proteins (alpha-1 B glycoprotein, afamin, apolipoprotein A1, apolipoprotein A4, Ig heavy constant a1, Ig heavy constant g4, leucine rich a2 glycoprotein 1, alpha-1 antitrypsin, antithrombin and transferrin) able to discriminate ABMR with good sensitivity and specificity using nano-reversed–phase liquid chromatography and shotgun mass spectrometry. These proteins were already described in other settings of kidney disease and are mainly reflecting general injury or injury mechanisms, rather than a specifically immunologically mediated process. This assay displayed a good negative predictive performance and was proposed as a screening tool for early diagnosis of ABMR with good confidence.
Urinary proteomic biomarkers are indeed very promising. However, until now, they have yet to reach widespread diagnostic use, which will likely rely on technology improvements and assay standardization (Fig. 1 and Table 1).
Non-invasive blood biomarkers
A large number of blood biomarkers have been studied using different methodologies, but only a few have reached clinical practice with assays available beyond the investigational context.
Donor-derived cell-free DNA
The term cell-free DNA (cfDNA) defines DNA fragments approximately 100–200 bp long, which are generated and released into the circulation by cells undergoing apoptosis. While this is a physiologic process, the amount of cfDNA may increase in conditions of cellular damage. In the field of transplantation, cellular injury of the graft derived from immune cell attack should result in a net increase of the amount of cfDNA of donor origin. In line with the notion that cfDNA is a marker of cellular injury, a rise in cfDNA may also be reflective of other causes of allograft injury, i.e., infection and acute tubular injury. Quantification of cfDNA of donor origin may therefore represent an effective and minimally invasive way to monitor rejection. In general, a positive correlation between high levels of donor-derived cfDNA (dd-cfDNA) and development of acute rejection was reported for lung, liver, heart, and kidney, including in pediatric recipients [67].
Even though this marker is promising, several areas of uncertainty remain. The first one concerns how to technically detect cfDNA: the principle behind dd-cfDNA quantification relies on the genetic differences between donor and recipient. The most accurate and sensitive methods are based on the analysis of panels of dozens or hundreds of single nucleotide polymorphisms (SNPs) performed using next-generation sequencing (NGS) approaches, which are quantitative. However, these methods are presently characterized by a long turnaround time of analysis and high costs, therefore limiting its application in the routine management of transplanted patients.
Given its high specificity and sensitivity in detecting donor DNA in a recipient’s blood, droplet digital PCR (ddPCR) is a valid alternative to NGS, providing a quantitative approach with contained costs [68].
The second area of uncertainty concerns how to quantify cfDNA and how to define an actionable threshold. The most common way to quantify cfDNA of the donor is as a percentage of the total. While this is a convenient method, it may be troublesome in the presence of infections, which can cause damage to the recipient affected cells and tissues, thereby increasing the total amount of recipient cfDNA and causing an underestimation of cfDNA of donor origin. The issue of the threshold remains perhaps the most critical point in the transfer of the assay in a clinical setting. In general, thresholds are dependent on the “total transplanted mass.” Consistently, the percentage of dd-cfDNA in liver transplanted patients is the highest, followed by lung, kidney, and heart.
The third area of uncertainty concerns how to use cfDNA: the issue of the value of cfDNA to monitor transplant rejection remains debatable [67]. In general, the great majority of studies highlight a positive correlation between the amount of cfDNA of donor origin and the presence of acute rejection. In addition, there seems to be an increase in dd-cfDNA levels in patients developing de novo DSA, suggesting that combined monitoring of dd-cfDNA and dnDSA may be more accurate in identifying patients undergoing ABMR and may help refine the patient population benefitting from a bioptic study of the graft [69].
Lastly, it has to be noted that the use of cell-free DNA in children poses additional problems, linked to the possibility of obtaining enough material from liquid biopsies and to optimizing cut-offs for this population. Recent data, however, have confirmed that in heart transplant recipients, children behave similarly to adults, with cfDNA being a very accurate predictor of rejection episodes [70, 71]. The experience with kidney transplants is far more limited, and more studies with larger patient cohorts and longer follow-up are needed determine the impact of dd-cfDNA monitoring during routine follow-up of kidney-transplanted patients (Fig. 1 and Table 1).
Peripheral blood transcriptomics
Peripheral blood gene expression profiling has also been used in independent studies to highlight a minimum set of genes that can predict rejection. In the Kidney Allograft Immune Biomarkers of Rejection Episodes (KALIBRE) study, Christakoudi and colleagues [72] studied by RT-qPCR the expression of 22 literature-based genes in peripheral blood samples from 248 patients. A 7-gene TCMR signature (IFNG, IP-10, ITGA4, MARCH8, RORc, SEMA7A, WDR40A) predicted rejection 7 weeks in advance of traditional markers. Furthermore, resolution of the rejection episode in response to therapy resulted in the return of gene expression levels to baseline values. Another study identified a 17-gene peripheral blood signature in patients with subclinical TCMR who received a protocol biopsy 3 months post-transplant within the GoCAR study (Genomics of Chronic Allograft Rejection) [73]. The targeted expression assay (TREx), validated in an external cohort, proved to have a high positive and negative predictive value over graft loss at 24 months.
In the multicenter prospective BIOMARGIN study, an 8-gene assay (CXCL10, FCGR1A, FCGR1B, GBP1, GBP4, IL15, KLRC1, TIMP1) was defined in a cohort of 49 patients with ABMR. This panel, validated in an independent cohort, proved to be of good diagnostic accuracy for times of stable graft function and of graft dysfunction, in the first and subsequent years. The 8-gene assay showed a good correlation with microvascular inflammation and transplant glomerulopathy, but not with the histological grade of the TCMR lesions [74].
The k-SORT (Kidney Solid Organ Response Test) 17-gene signature was defined in the multicenter Assessment of Acute Rejection in Renal Transplant (AART) study, also including a cohort of children: this assay proved predictive with a 93% positive predictive value, of both TCMR and ABMR 3 months before biopsy in the discovery and the validation cohort [75]. In another recent study, retrospectively recruiting 1763 samples from a multicenter biobank, the k-SORT assay did not reach the diagnostic value displayed in the discovery cohort [76].
The CTOT-08 prospective multicenter trial enrolled adults on a surveillance biopsy protocol and used a 57-gene expression profile signature that efficiently discriminated between stable grafts without histological signs of rejection and subclinical rejection at 24 months with good accuracy. Thanks to the elevated negative predictive value for subclinical acute rejection (NPV 88%), this assay would potentially allow avoiding unnecessary biopsies in patients with negative results [77]. These data were confirmed in an independent study [78]. This test is available as TruGraf® and is performed by the producer (Eurofins-Viracor, Transplant Genomics Inc. USA). However, to date, it has not been cleared or approved for diagnostic use by the US Food and Drug Administration (Fig. 1 and Table 1).
Blood proteomics
The identification of blood proteins with biomarker significance requires a high resolving fractionating method, to be able to fish informative proteins at extremely low concentrations and overcome the confounding prevailing presence of plasma proteins deriving from normal tissue homeostasis.
Cibrik et al. [79] identified a “protein signature” able to discriminate between stable transplant patients and those with rejection. Of the 17 proteins that define the signature, in the rejecting cohort, nine had lower expression (E-cadherin, EGF, erythropoietin receptor, growth regulated oncogene-alpha, interleukin 6, MCP-1 macrophage inflammatory protein 3-alpha, transforming growth factor β 1 and 2) and eight higher (GM-CSF, interleukin 1 receptor 1, interleukin 12 p70, KIM-1, MIF, osteopontin, tumor necrosis factor receptor II, and vascular endothelial growth factor receptor). While interesting, this approach remains inconclusive due to the methodological limitations of a cohort study on indication biopsy and the choice of protein set based on the available antibodies. Other studies, including retrospective cohorts studied with a combination of IL-1 receptor antagonist, IL-20, and sCD40L or panels of other proteins or soluble co-stimulatory molecules such as CD30, are extensively reviewed elsewhere (Fig. 1 and Table 1).
Peripheral blood EVs
Extracellular vesicles (EVs) derived from plasma have been investigated so far only in a few non-cross-validated studies [40] due to the higher technical complexity required for proper characterization, being > 70% of lymphoid origin and possibly masking signals derived from graft cells.
In a small cohort study of 28 adults, plasma density of EVs with surface expression of C4d/CD144, as marker of endothelial injury, was associated with ABMR, correlated to biopsy severity and was modulated by rejection treatment [80]. Another small study of 64 adult patients (18 ABMR and 8 TCMR) identified in plasma EVs a gene expression combination score of 4 genes (gp130, SH2D1B, TNFα, and CCL4) significantly higher in the ABMR than TCMR subjects [81]. While EVs appear a versatile tool to explore the immunological and inflammatory mechanisms of allorecognition, methodological complexities need to be addressed before they can be considered a widely applicable biomarker (Fig. 1 and Table 1).
Markers of immune status: virus specific T cells and torque teno virus
The assessment of virus-specific T cells (Tvis) is a functional marker of immunosuppression that was prospectively investigated in a pediatric phase 2 randomized multicenter study. Serial assessment of CD4 Tvis against adenovirus, cytomegalovirus, and herpes symplex virus allowed personalized steering of immunosuppressive therapy with a net reduction of the exposure to unnecessary overimmunosuppression, reduced infection events, and comparable kidney function [82].
Another approach, leading to conceptually similar information, is the quantitative assay of torque teno virus (TTV) load, which allows one to simplify the complex laboratory technique used for Tvis analysis. TTV is a non-pathogenic virus present in the majority of individuals, with increasing replication in parallel to the increase of immunosuppression status. TTV load can represent a direct biomarker of the immune status, being potentially useful to steer drug dosage to target the proper balance between rejection and excess infection, with good performance [83]. Two randomized prospective interventional trials are ongoing.
Conclusions
Allorecognition is a complex phenomenon that cannot be thoroughly captured by the traditional biomarkers in use, which measure organ function, but generally fail to predict rejection before it becomes clinically evident. Recent experimental approaches have highlighted novel possibilities that will allow us to monitor graft health, modulate levels of immunosuppression, and ultimately to eliminate or reduce the need for protocol biopsies.
Even if these approaches have been successful in several clinical trials, they still need to reach wide clinical application. This is particularly true in the pediatric setting, where the small patient numbers often preclude systematic testing of novel assays to diagnose rejection. Large and validated studies, addressing also the pediatric population, are therefore needed to take advantage of these highly versatile tools non-invasively and longitudinally over the long run.
References
Sellares J, de Freitas DG, Mengel M, Reeve J, Einecke G, Sis B, Hidalgo LG, Famulski K, Matas A, Halloran PF (2012) Understanding the causes of kidney transplant failure: the dominant role of antibody-mediated rejection and nonadherence. Am J Transplant 12:388–399
Gordillo R, Munshi R, Monroe EJ, Shivaram GM, Smith JM (2019) Benefits and risks of protocol biopsies in pediatric renal transplantation. Pediatr Nephrol 34:593–598
Barton KT, Halani K, Galbiati S, Dandamudi R, Hmiel SP, Dharnidharka VR, NAPRTCS investigators (2021) Late first acute rejection in pediatric kidney transplantation: a North American Pediatric Renal Trials and collaborative studies special study. Pediatr Transplant 25:e13953
Kanzelmeyer NK, Lerch C, Ahlenstiel-Grunow T, Brasen JH, Haffner D, Pape L (2020) The role of protocol biopsies after pediatric kidney transplantation. Medicine (Baltimore) 99:e20522
Moudgil A, Martz K, Stablein DM, Puliyanda DP (2010) Variables affecting estimated glomerular filtration rate after renal transplantation in children: a NAPRTCS data analysis. Pediatr Transplant 14:288–294
Naesens M, Lerut E, Emonds MP, Herelixka A, Evenepoel P, Claes K, Bammens B, Sprangers B, Meijers B, Jochmans I, Monbaliu D, Pirenne J, Kuypers DR (2016) Proteinuria as a noninvasive marker for renal allograft histology and failure: an observational cohort study. J Am Soc Nephrol 27:281–292
Kanzelmeyer NK, Ahlenstiel T, Drube J, Froede K, Kreuzer M, Broecker V, Ehrich JH, Melk A, Pape L (2010) Protocol biopsy-driven interventions after pediatric renal transplantation. Pediatr Transplant 14:1012–1018
Zotta F, Guzzo I, Morolli F, Diomedi-Camassei F, Dello Strologo L (2018) Protocol biopsies in pediatric renal transplantation: a precious tool for clinical management. Pediatr Nephrol 33:2167–2175
Lee DM, Abecassis MM, Friedewald JJ, Rose S, First MR (2020) Kidney graft surveillance biopsy utilization and trends: results from a survey of high-volume transplant centers. Transplant Proc 52:3085–3089
Hoffmann AJ, Gibson IW, Ho J, Nickerson P, Rush D, Sharma A, Wishart D, Blydt-Hansen TD (2021) Early surveillance biopsy utilization and management of pediatric renal allograft acute T cell-mediated rejection in Canadian centers: observations from the PROBE multicenter cohort study. Pediatr Transplant 25:e13870
Bergan S, Brunet M, Hesselink DA, Johnson-Davis KL, Kunicki PK, Lemaitre F, Marquet P, Molinaro M, Noceti O, Pattanaik S, Pawinski T, Seger C, Shipkova M, Swen JJ, van Gelder T, Venkataramanan R, Wieland E, Woillard JB, Zwart TC, Barten MJ, Budde K, Dieterlen MT, Elens L, Haufroid V, Masuda S, Millan O, Mizuno T, Moes D, Oellerich M, Picard N, Salzmann L, Tonshoff B, van Schaik RHN, Vethe NT, Vinks AA, Wallemacq P, Asberg A, Langman LJ (2021) Personalized therapy for mycophenolate: consensus report by the International Association of Therapeutic Drug Monitoring and Clinical Toxicology. Ther Drug Monit 43:150–200
Kuypers DRJ (2020) Intrapatient variability of tacrolimus exposure in solid organ transplantation: a novel marker for clinical outcome. Clin Pharmacol Ther 107:347–358
Eid L, Tuchman S, Moudgil A (2014) Late acute rejection: incidence, risk factors, and effect on graft survival and function. Pediatr Transplant 18:155–162
Pollock-Barziv SM, Finkelstein Y, Manlhiot C, Dipchand AI, Hebert D, Ng VL, Solomon M, McCrindle BW, Grant D (2010) Variability in tacrolimus blood levels increases the risk of late rejection and graft loss after solid organ transplantation in older children. Pediatr Transplant 14:968–975
Marquet P, Cros F, Micallef L, Jacqz-Aigrain E, Woillard JB, Monchaud C, Saint-Marcoux F, Debord J (2021) Tacrolimus Bayesian dose adjustment in pediatric renal transplant recipients. Ther Drug Monit 43:472–480
Davis S, Gralla J, Klem P, Tong S, Wedermyer G, Freed B, Wiseman A, Cooper JE (2018) Lower tacrolimus exposure and time in therapeutic range increase the risk of de novo donor-specific antibodies in the first year of kidney transplantation. Am J Transplant 18:907–915
Chong AS (2020) Mechanisms of organ transplant injury mediated by B cells and antibodies: Implications for antibody-mediated rejection. Am J Transplant 20(Suppl 4):23–32
Kim JJ, Balasubramanian R, Michaelides G, Wittenhagen P, Sebire NJ, Mamode N, Shaw O, Vaughan R, Marks SD (2014) The clinical spectrum of de novo donor-specific antibodies in pediatric renal transplant recipients. Am J Transplant 14:2350–2358
Ginevri F, Nocera A, Comoli P, Innocente A, Cioni M, Parodi A, Fontana I, Magnasco A, Nocco A, Tagliamacco A, Sementa A, Ceriolo P, Ghio L, Zecca M, Cardillo M, Garibotto G, Ghiggeri GM, Poli F (2012) Posttransplant de novo donor-specific hla antibodies identify pediatric kidney recipients at risk for late antibody-mediated rejection. Am J Transplant 12:3355–3362
Pape L, Becker JU, Immenschuh S, Ahlenstiel T (2015) Acute and chronic antibody-mediated rejection in pediatric kidney transplantation. Pediatr Nephrol 30:417–424
Loupy A, Lefaucheur C, Vernerey D, Prugger C, Duong van Huyen JP, Mooney N, Suberbielle C, Fremeaux-Bacchi V, Mejean A, Desgrandchamps F, Anglicheau D, Nochy D, Charron D, Empana JP, Delahousse M, Legendre C, Glotz D, Hill GS, Zeevi A, Jouven X (2013) Complement-binding anti-HLA antibodies and kidney-allograft survival. N Engl J Med 369:1215–1226
Heilman RL, Nijim A, Desmarteau YM, Khamash H, Pando MJ, Smith ML, Chakkera HA, Huskey J, Valdez R, Reddy KS (2014) De novo donor-specific human leukocyte antigen antibodies early after kidney transplantation. Transplantation 98:1310–1315
Ding Y, Francis J, Gautam A, Pelletier L, Sanchorawala V, Quillen K (2018) Durable renal response after combination of bortezomib, corticosteroids, rituximab, and plasmapheresis for late antibody-mediated renal transplant rejection. Clin Nephrol 89:252–259
O’Leary JG, Samaniego M, Crespo Barrio M, Potena L, Zeevi A, Djamali A, Cozzi E (2016) The influence of immunosuppressive agents on the risk of de novo donor-specific hla antibody production in solid organ transplant recipients. Transplantation 100:39–53
Filler G, Todorova EK, Bax K, Alvarez-Elias AC, Huang SH, Kobrzynski MC (2016) Minimum mycophenolic acid levels are associated with donor-specific antibody formation. Pediatr Transplant 20:34–38
Cioni M, Comoli P, Tagliamacco A, Innocente A, Basso S, Fontana I, Magnasco A, Trivelli A, Nocco A, Macchiagodena M, Catenacci L, Klersy C, Verrina E, Garibotto G, Ghiggeri GM, Cardillo M, Ginevri F, Nocera A (2021) Post-transplant de novo non donor-specific HLA antibodies are not associated with poor graft outcome in non-sensitized pediatric recipients of kidney transplantation. Transpl Immunol 65:101375
Wiebe C, Gibson IW, Blydt-Hansen TD, Karpinski M, Ho J, Storsley LJ, Goldberg A, Birk PE, Rush DN, Nickerson PW (2012) Evolution and clinical pathologic correlations of de novo donor-specific HLA antibody post kidney transplant. Am J Transplant 12:1157–1167
Hourmant M, Cesbron-Gautier A, Terasaki PI, Mizutani K, Moreau A, Meurette A, Dantal J, Giral M, Blancho G, Cantarovich D, Karam G, Follea G, Soulillou JP, Bignon JD (2005) Frequency and clinical implications of development of donor-specific and non-donor-specific HLA antibodies after kidney transplantation. J Am Soc Nephrol 16:2804–2812
Terasaki PI, Ozawa M, Castro R (2007) Four-year follow-up of a prospective trial of HLA and MICA antibodies on kidney graft survival. Am J Transplant 7:408–415
Susal C, Wettstein D, Dohler B, Morath C, Ruhenstroth A, Scherer S, Tran TH, Gombos P, Schemmer P, Wagner E, Fehr T, Zivcic-Cosic S, Balen S, Weimer R, Slavcev A, Bosmuller C, Norman DJ, Zeier M, Opelz G, Collaborative Transplant Study Report (2015) Association of kidney graft loss with de novo produced donor-specific and non-donor-specific HLA antibodies detected by single antigen testing. Transplantation 99:1976–1980
Einecke G, Sis B, Reeve J, Mengel M, Campbell PM, Hidalgo LG, Kaplan B, Halloran PF (2009) Antibody-mediated microcirculation injury is the major cause of late kidney transplant failure. Am J Transplant 9:2520–2531
Fichtner A, Susal C, Hocker B, Rieger S, Waldherr R, Westhoff JH, Sander A, Dragun D, Tonshoff B (2021) Association of non-HLA antibodies against endothelial targets and donor-specific HLA antibodies with antibody-mediated rejection and graft function in pediatric kidney transplant recipients. Pediatr Nephrol 36:2473–2484
Dragun D, Muller DN, Brasen JH, Fritsche L, Nieminen-Kelha M, Dechend R, Kintscher U, Rudolph B, Hoebeke J, Eckert D, Mazak I, Plehm R, Schonemann C, Unger T, Budde K, Neumayer HH, Luft FC, Wallukat G (2005) Angiotensin II type 1-receptor activating antibodies in renal-allograft rejection. N Engl J Med 352:558–569
Pearl MH, Zhang Q, Palma Diaz MF, Grotts J, Rossetti M, Elashoff D, Gjertson DW, Weng P, Reed EF, Tsai Chambers E (2018) Angiotensin II Type 1 receptor antibodies are associated with inflammatory cytokines and poor clinical outcomes in pediatric kidney transplantation. Kidney Int 93:260–269
Halloran PF, Venner JM, Famulski KS (2017) Comprehensive analysis of transcript changes associated with allograft rejection: combining universal and selective features. Am J Transplant 17:1754–1769
Halloran PF, Pereira AB, Chang J, Matas A, Picton M, De Freitas D, Bromberg J, Seron D, Sellares J, Einecke G, Reeve J (2013) Potential impact of microarray diagnosis of T cell-mediated rejection in kidney transplants: The INTERCOM study. Am J Transplant 13:2352–2363
Halloran PF, Pereira AB, Chang J, Matas A, Picton M, De Freitas D, Bromberg J, Seron D, Sellares J, Einecke G, Reeve J (2013) Microarray diagnosis of antibody-mediated rejection in kidney transplant biopsies: an international prospective study (INTERCOM). Am J Transplant 13:2865–2874
Mengel M, Loupy A, Haas M, Roufosse C, Naesens M, Akalin E, Clahsen-van Groningen MC, Dagobert J, Demetris AJ, Duong van Huyen JP, Gueguen J, Issa F, Robin B, Rosales I, Von der Thusen JH, Sanchez-Fueyo A, Smith RN, Wood K, Adam B, Colvin RB (2020) Banff 2019 Meeting Report: Molecular diagnostics in solid organ transplantation-consensus for the Banff Human Organ Transplant (B-HOT) gene panel and open source multicenter validation. Am J Transplant 20:2305–2317
O’Connell PJ, Zhang W, Menon MC, Yi Z, Schröppel B, Gallon L, Luan Y, Rosales IA, Ge Y, Losic B, Xi C, Woytovich C, Keung KL, Wei C, Greene I, Overbey J, Bagiella E, Najafian N, Samaniego M, Djamali A, Alexander SI, Nankivell BJ, Chapman JR, Smith RN, Colvin R, Murphy B (2016) Biopsy transcriptome expression profiling to identify kidney transplants at risk of chronic injury: a multicentre, prospective study. Lancet 388:983–993
Ashcroft J, Leighton P, Elliott TR, Hosgood SA, Nicholson ML, Kosmoliaptsis V (2022) Extracellular vesicles in kidney transplantation: a state-of-the-art review. Kidney Int 101:485–497
Sigdel TK, Ng YW, Lee S, Nicora CD, Qian WJ, Smith RD, Camp DG 2nd, Sarwal MM (2014) Perturbations in the urinary exosome in transplant rejection. Front Med (Lausanne) 1:57
Lim JH, Lee CH, Kim KY, Jung HY, Choi JY, Cho JH, Park SH, Kim YL, Baek MC, Park JB, Kim YH, Chung BH, Lee SH, Kim CD (2018) Novel urinary exosomal biomarkers of acute T cell-mediated rejection in kidney transplant recipients: a cross-sectional study. PLoS One 13:e0204204
Jung HY, Lee CH, Choi JY, Cho JH, Park SH, Kim YL, Moon PG, Baek MC, Berm Park J, Hoon Kim Y, Ha Chung B, Lee SH, Kim CD (2020) Potential urinary extracellular vesicle protein biomarkers of chronic active antibody-mediated rejection in kidney transplant recipients. J Chromatogr B Analyt Technol Biomed Life Sci 1138:121958
Park J, Lin HY, Assaker JP, Jeong S, Huang CH, Kurdi T, Lee K, Fraser K, Min C, Eskandari S, Routray S, Tannous B, Abdi R, Riella L, Chandraker A, Castro CM, Weissleder R, Lee H, Azzi JR (2017) Integrated kidney exosome analysis for the detection of kidney transplant rejection. ACS Nano 11:11041–11046
El Fekih R, Hurley J, Tadigotla V, Alghamdi A, Srivastava A, Coticchia C, Choi J, Allos H, Yatim K, Alhaddad J, Eskandari S, Chu P, Mihali AB, Lape IT, Lima Filho MP, Aoyama BT, Chandraker A, Safa K, Markmann JF, Riella LV, Formica RN, Skog J, Azzi JR (2021) Discovery and validation of a urinary exosome mRNA signature for the diagnosis of human kidney transplant rejection. J Am Soc Nephrol 32:994–1004
Suthanthiran M, Schwartz JE, Ding R, Abecassis M, Dadhania D, Samstein B, Knechtle SJ, Friedewald J, Becker YT, Sharma VK, Williams NM, Chang CS, Hoang C, Muthukumar T, August P, Keslar KS, Fairchild RL, Hricik DE, Heeger PS, Han L, Liu J, Riggs M, Ikle DN, Bridges ND, Shaked A, Clinical Trials in Organ Transplantation 04 (CTOT-04) Study Investigators (2013) Urinary-cell mRNA profile and acute cellular rejection in kidney allografts. N Engl J Med 369:20–31
Matignon M, Ding R, Dadhania DM, Mueller FB, Hartono C, Snopkowski C, Li C, Lee JR, Sjoberg D, Seshan SV, Sharma VK, Yang H, Nour B, Vickers AJ, Suthanthiran M, Muthukumar T (2014) Urinary cell mRNA profiles and differential diagnosis of acute kidney graft dysfunction. J Am Soc Nephrol 25:1586–1597
Sigdel T, Nguyen M, Liberto J, Dobi D, Junger H, Vincenti F, Laszik Z, Sarwal MM (2019) Assessment of 19 genes and validation of CRM gene panel for quantitative transcriptional analysis of molecular rejection and inflammation in archival kidney transplant biopsies. Front Med 6:213
Hricik DE, Nickerson P, Formica RN, Poggio ED, Rush D, Newell KA, Goebel J, Gibson IW, Fairchild RL, Riggs M, Spain K, Ikle D, Bridges ND, Heeger PS, CTOT-10 consortium (2013) Multicenter validation of urinary CXCL9 as a risk-stratifying biomarker for kidney transplant injury. Am J Transplant 13:2634–2644
Kaminski MM, Alcantar MA, Lape IT, Greensmith R, Huske AC, Valeri JA, Marty FM, Klambt V, Azzi J, Akalin E, Riella LV, Collins JJ (2020) A CRISPR-based assay for the detection of opportunistic infections post-transplantation and for the monitoring of transplant rejection. Nat Biomed Eng 4:601–609
Lorenzen JM, Volkmann I, Fiedler J, Schmidt M, Scheffner I, Haller H, Gwinner W, Thum T (2011) Urinary miR-210 as a mediator of acute T-cell mediated rejection in renal allograft recipients. Am J Transplant 11:2221–2227
Millan O, Budde K, Sommerer C, Aliart I, Rissling O, Bardaji B, Matz M, Zeier M, Silva I, Guirado L, Brunet M (2017) Urinary miR-155-5p and CXCL10 as prognostic and predictive biomarkers of rejection, graft outcome and treatment response in kidney transplantation. Br J Clin Pharmacol 83:2636–2650
Gielis EM, Anholts JDH, van Beelen E, Haasnoot GW, De Fijter HW, Bajema I, Heidt S, van de Vrie M, Hilbrands LB, Mallat MJK, Ledeganck KJ, Claas FHJ, Eikmans M (2021) A combined microRNA and chemokine profile in urine to identify rejection after kidney transplantation. Transplant Direct 7:e711
Jackson JA, Kim EJ, Begley B, Cheeseman J, Harden T, Perez SD, Thomas S, Warshaw B, Kirk AD (2011) Urinary chemokines CXCL9 and CXCL10 are noninvasive markers of renal allograft rejection and BK viral infection. Am J Transplant 11:2228–2234
Blydt-Hansen TD, Gibson IW, Gao A, Dufault B, Ho J (2015) Elevated urinary CXCL10-to-creatinine ratio is associated with subclinical and clinical rejection in pediatric renal transplantation. Transplantation 99:797–804
Mockler C, Sharma A, Gibson IW, Gao A, Wong A, Ho J, Blydt-Hansen TD (2018) The prognostic value of urinary chemokines at 6 months after pediatric kidney transplantation. Pediatr Transplant 22:e13205
Mincham CM, Gibson IW, Sharma A, Wiebe C, Mandal R, Rush D, Nickerson P, Ho J, Wishart DS, Blydt-Hansen TD (2018) Evolution of renal function and urinary biomarker indicators of inflammation on serial kidney biopsies in pediatric kidney transplant recipients with and without rejection. Pediatr Transplant 22:e13202
Blydt-Hansen TD, Sharma A, Gibson IW, Wiebe C, Sharma AP, Langlois V, Teoh CW, Rush D, Nickerson P, Wishart D, Ho J (2021) Validity and utility of urinary CXCL10/Cr immune monitoring in pediatric kidney transplant recipients. Am J Transplant 21:1545–1555
Kumar J, Contrepois K, Snyder M, Grimm PC, Moudgil A, Smith JM, Bobrowski AE, Verghese PS, Hooper D, Ingulli E, Lestz R, Weng P, Reason JL, Blydt-Hansen TD, Suthanthiran M, Keating B, Amaral S (2021) Design and Methods of the Validating Injury to the Renal Transplant Using Urinary Signatures (VIRTUUS) study in children. Transplant Direct 7:e791
Blydt-Hansen TD, Sharma A, Gibson IW, Mandal R, Wishart DS (2014) Urinary metabolomics for noninvasive detection of borderline and acute T cell-mediated rejection in children after kidney transplantation. Am J Transplant 14:2339–2349
Banas M, Neumann S, Eiglsperger J, Schiffer E, Putz FJ, Reichelt-Wurm S, Kramer BK, Pagel P, Banas B (2018) Identification of a urine metabolite constellation characteristic for kidney allograft rejection. Metabolomics 14:116
Banas MC, Bohmig GA, Viklicky O, Rostaing LP, Jouve T, Guirado L, Facundo C, Bestard O, Grone HJ, Kobayashi K, Hanzal V, Putz FJ, Zecher D, Bergler T, Neumann S, Rothe V, Schwable Santamaria AG, Schiffer E, Banas B (2021) A prospective multicenter trial to evaluate Urinary Metabolomics for Non-invasive Detection of Renal Allograft Rejection (PARASOL): study Protocol and Patient Recruitment. Front Med (Lausanne) 8:780585
Yang JYC, Sarwal RD, Sigdel TK, Damm I, Rosenbaum B, Liberto JM, Chan-On C, Arreola-Guerra JM, Alberu J, Vincenti F, Sarwal MM (2020) A urine score for noninvasive accurate diagnosis and prediction of kidney transplant rejection. Sci Transl Med 12(535):eaba2501. https://doi.org/10.1126/scitranslmed.aba2501
Kanzelmeyer NK, Zurbig P, Mischak H, Metzger J, Fichtner A, Ruszai KH, Seemann T, Hansen M, Wygoda S, Krupka K, Tonshoff B, Melk A, Pape L (2019) Urinary proteomics to diagnose chronic active antibody-mediated rejection in pediatric kidney transplantation - a pilot study. Transpl Int 32:28–37
Naesens M, Friedewald J, Mas V, Kaplan B, Abecassis MM (2020) A practical guide to the clinical implementation of biomarkers for subclinical rejection following kidney transplantation. Transplantation 104:700–707
Mertens I, Willems H, Van Loon E, Schildermans K, Boonen K, Baggerman G, Valkenborg D, Gwinner W, Anglicheau D, Essig M, Marquet P, Naesens M (2020) Urinary protein biomarker panel for the diagnosis of antibody-mediated rejection in kidney transplant recipients. Kidney Int Rep 5:1448–1458
Steggerda JA, Pizzo H, Garrison J, Zhang X, Haas M, Kim IK, Jordan SC, Puliyanda DP (2022) Use of a donor-derived cell-free DNA assay to monitor treatment response in pediatric renal transplant recipients with allograft rejection. Pediatr Transplant 26:e14258
Sorbini M, Togliatto GM, Simonato E, Boffini M, Cappuccio M, Gambella A, Arruga F, Mora N, Marro M, Caorsi C, Mansouri M, Magistroni P, Delsedime L, Papotti MG, Amoroso A, Rinaldi M, Vaisitti T, Deaglio S (2021) HLA-DRB1 mismatch-based identification of donor-derived cell free DNA (dd-cfDNA) as a marker of rejection in heart transplant recipients: a single-institution pilot study. J Heart Lung Transplant 40:794–804
Zhang H, Liu L, Zheng C, Li X, Fu Q, Li J, Su Q, Huang H, Ye M, Wang C (2018) The role of donor-derived cell-free DNA in the identification of injury in kidney allografts with antibody-mediated rejection or de novo DSA. Transplantation 102:S5–S6
Zangwill SD, Deshpande SR, Simpson PM, Liang HL, Zhang L, Dasgupta M, Richmond ME, Kindel SJ, Bichell DP, Mahle WT, Wigger MA, Schroder JN, Knecht KR, Pahl E, Gaglianello NA, North PE, Tomita-Mitchell A, Mitchell ME (2022) Increase in nuclear cell-free DNA is associated with major adverse events in adult and pediatric heart transplant recipients. Clin Transplant 36:e14509
Richmond ME, Zangwill SD, Kindel SJ, Deshpande SR, Schroder JN, Bichell DP, Knecht KR, Mahle WT, Wigger MA, Gaglianello NA, Pahl E, Simpson PM, Dasgupta M, North PE, Hidestrand M, Tomita-Mitchell A, Mitchell ME (2020) Donor fraction cell-free DNA and rejection in adult and pediatric heart transplantation. J Heart Lung Transplant 39:454–463
Christakoudi S, Runglall M, Mobillo P, Tsui TL, Duff C, Domingo-Vila C, Kamra Y, Delaney F, Montero R, Spiridou A, Kassimatis T, Phin-Kon S, Tucker B, Farmer C, Strom TB, Lord GM, Rebollo-Mesa I, Stahl D, Sacks S, Hernandez-Fuentes MP, Chowdhury P (2019) Development of a multivariable gene-expression signature targeting T-cell-mediated rejection in peripheral blood of kidney transplant recipients validated in cross-sectional and longitudinal samples. EBioMedicine 41:571–583
Zhang W, Yi Z, Keung KL, Shang H, Wei C, Cravedi P, Sun Z, Xi C, Woytovich C, Farouk S, Huang W, Banu K, Gallon L, Magee CN, Najafian N, Samaniego M, Djamali A, Alexander SI, Rosales IA, Smith RN, Xiang J, Lerut E, Kuypers D, Naesens M, O’Connell PJ, Colvin R, Menon MC, Murphy B (2019) A peripheral blood gene expression signature to diagnose subclinical acute rejection. J Am Soc Nephrol 30:1481–1494
Van Loon E, Gazut S, Yazdani S, Lerut E, de Loor H, Coemans M, Noel LH, Thorrez L, Van Lommel L, Schuit F, Sprangers B, Kuypers D, Essig M, Gwinner W, Anglicheau D, Marquet P, Naesens M (2019) Development and validation of a peripheral blood mRNA assay for the assessment of antibody-mediated kidney allograft rejection: a multicentre, prospective study. EBioMedicine 46:463–472
Roedder S, Sigdel T, Salomonis N, Hsieh S, Dai H, Bestard O, Metes D, Zeevi A, Gritsch A, Cheeseman J, Macedo C, Peddy R, Medeiros M, Vincenti F, Asher N, Salvatierra O, Shapiro R, Kirk A, Reed EF, Sarwal MM (2014) The kSORT assay to detect renal transplant patients at high risk for acute rejection: results of the multicenter AART study. PLoS Med 11:e1001759
Van Loon E, Giral M, Anglicheau D, Lerut E, Dubois V, Rabeyrin M, Brouard S, Roedder S, Spigarelli MG, Rabant M, Bogaerts K, Naesens M, Thaunat O (2021) Diagnostic performance of kSORT, a blood-based mRNA assay for noninvasive detection of rejection after kidney transplantation: a retrospective multicenter cohort study. Am J Transplant 21:740–750
Friedewald JJ, Kurian SM, Heilman RL, Whisenant TC, Poggio ED, Marsh C, Baliga P, Odim J, Brown MM, Ikle DN, Armstrong BD, Charette JI, Brietigam SS, Sustento-Reodica N, Zhao L, Kandpal M, Salomon DR, Abecassis MM, Clinical Trials in Organ Transplantation 08 (CTOT-08) (2019) Development and clinical validity of a novel blood-based molecular biomarker for subclinical acute rejection following kidney transplant. Am J Transplant 19:98–109
Ang A, Schieve C, Rose S, Kew C, First MR, Mannon RB (2021) Avoiding surveillance biopsy: use of a noninvasive biomarker assay in a real-life scenario. Clin Transplant 35:e14145
Cibrik DM, Warner RL, Kommareddi M, Song P, Luan FL, Johnson KJ (2013) Identification of a protein signature in renal allograft rejection. Proteomics Clin Appl 7:839–849
Tower CM, Reyes M, Nelson K, Leca N, Kieran N, Muczynski K, Jefferson JA, Blosser C, Kukla A, Maurer D, Chandler W, Najafian B (2017) Plasma C4d+ endothelial microvesicles increase in acute antibody-mediated rejection. Transplantation 101:2235–2243
Zhang H, Huang E, Kahwaji J, Nast CC, Li P, Mirocha J, Thomas DL, Ge S, Vo AA, Jordan SC, Toyoda M (2017) Plasma exosomes from HLA-sensitized kidney transplant recipients contain mRNA transcripts which predict development of antibody-mediated rejection. Transplantation 101:2419–2428
Ahlenstiel-Grunow T, Liu X, Schild R, Oh J, Taylan C, Weber LT, Staude H, Verboom M, Schroder C, Sabau R, Grosshennig A, Pape L (2021) Steering transplant immunosuppression by measuring virus-specific T cell levels: the randomized, controlled IVIST trial. J Am Soc Nephrol 32:502–516
Jaksch P, Gorzer I, Puchhammer-Stockl E, Bond G (2022) Integrated immunologic monitoring in solid organ transplantation: the road towards torque teno virus-guided immunosuppression. Transplantation 106:1940–1951
Acknowledgements
The help of Dr. Vitor Hugo Martins, University of Turin, and the suggestions of Prof. Umberto Maggiore, University of Parma Italy, are acknowledged. This work was generated within the European Reference Network TransplantChild.
Funding
Open access funding provided by Università degli Studi di Torino within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Peruzzi, L., Deaglio, S. Rejection markers in kidney transplantation: do new technologies help children?. Pediatr Nephrol 38, 2939–2955 (2023). https://doi.org/10.1007/s00467-022-05872-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-022-05872-z