
Abstract
Background
Baseline serum creatinine (bSCr) is required for diagnosing acute kidney injury (AKI). In children, bSCr is commonly defined as the lowest measurement within 3 months of admission. Measured values are often missing and estimating bSCr using height-based glomerular filtration rate (GFR) equations is problematic when height is unavailable.
Methods
This is a retrospective cohort study including 538 children admitted to the intensive care unit (ICU) between 2003 and 2005 at two centers in Canada, with measured bSCr, height, and ICU-SCr values. We evaluated the bias, accuracy, and precision of back-calculating bSCr from height-dependent and height-independent GFR equations. Agreement of AKI defined using measured and estimated bSCr was calculated. Multivariate analyses were performed to assess the impact of bSCr estimation methods on the association between AKI and ICU mortality, length of stay, and duration of mechanical ventilation.
Results
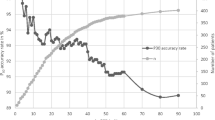
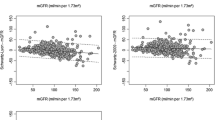
Both methods underestimated bSCr by 1–3%, showed good accuracy (∼30% of patients with estimated bSCr within 10% of measured bSCr), but poor precision (wide 95% limits of agreement). The agreement between AKI defined by estimated versus measured bSCr was >80% (κ >0.5). The height-independent method performed best in children >13 years old; however, overall, both methods performed similarly across age subgroups. AKI was associated with longer stay, prolonged mechanical ventilation, and ICU mortality using measured and estimated bSCr.
Conclusions
Height-dependent and height-independent bSCr estimation methods were comparable. This may have significant implications for performing pediatric AKI research using large databases, and in clinical care to define AKI when height is unknown.


Similar content being viewed by others

References
Alkandari O, Eddington KA, Hyder A, Gauvin F, Ducruet T, Gottesman R, Phan V, Zappitelli M (2011) Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: a two-center retrospective cohort study. Crit Care 15:R146
Schneider J, Khemani R, Grushkin C, Bart R (2010) Serum creatinine as stratified in the RIFLE score for acute kidney injury is associated with mortality and length of stay for children in the pediatric intensive care unit. Crit Care Med 38:933–939
Soler YA, Nieves-Plaza M, Prieto M, García-De Jesús R, Suárez-Rivera M (2013) pRIFLE (Pediatric Risk, Injury, Failure, Loss, End Stage Renal Disease) score identifies acute kidney injury and predicts mortality in critically ill children: a prospective study. Pediatr Crit Care Med 14:e189–e195
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group (2012) KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl 2:1–138
Bresolin N, Bianchini AP, Haas CA (2013) Pediatric acute kidney injury assessed by pRIFLE as a prognostic factor in the intensive care unit. Pediatr Nephrol 28:485–492
Kavaz A, Ozcakar ZB, Kendirli T, Ozturk BB, Ekim M, Yalcinkaya F (2012) Acute kidney injury in a paediatric intensive care unit: comparison of the pRIFLE and AKIN criteria. Acta Paediatr 101:e126–e129
Prodhan P, McCage LS, Stroud MH, Gossett J, Garcia X, Bhutta AT, Schexnayder S, Maxson RT, Blaszak RT (2012) Acute kidney injury is associated with increased in-hospital mortality in mechanically ventilated children with trauma. J Trauma Acute Care Surg. 73:832–837
Selewski DT, Cornell TT, Heung M, Troost JP, Ehrmann BJ, Lombel RM, Blatt NB, Luckritz K, Hieber S, Gajarski R, Kershaw DB, Shanley TP, Gipson DS (2014) Validation of the KDIGO acute kidney injury criteria in a pediatric critical care population. Intensive Care Med 40:1481–1488
Zappitelli M, Parikh CR, Akcan-Arikan A, Washburn KK, Moffett BS, Goldstein SL (2008) Ascertainment and epidemiology of acute kidney injury varies with definition interpretation. Clin J Am Soc Nephrol 3:948–954
Volpon LC, Sugo EK, Consulin JC, Tavares TL, Aragon DC, Carlotti AP (2016) Epidemiology and outcome of acute kidney injury according to Pediatric Risk, Injury, Failure, Loss, End-Stage Renal Disease and Kidney Disease: Improving Global Outcomes criteria in critically ill children-A prospective study. Pediatr Crit Care Med 17:e229–e238
Thongprayoon C, Cheungpasitporn W, Harrison AM, Kittanamongkolchai W, Ungprasert P, Srivali N, Akhoundi A, Kashani KB (2016) The comparison of the commonly used surrogates for baseline renal function in acute kidney injury diagnosis and staging. BMC Nephrol 17:6
Sanchez-Pinto LN, Goldstein SL, Schneider JB, Khemani RG (2015) Association between progression and improvement of acute kidney injury and mortality in critically ill children. Pediatr Crit Care Med 16:703–710
Hayton WL (2000) Maturation and growth of renal function: dosing renally cleared drugs in children. AAPS PharmSci 2:E3
Cabral FC, Ramos Garcia PC, Mattiello R, Dresser D, Fiori HH, Korb C, Dalcin TC, Piva JP (2015) Influence of acute kidney injury defined by the Pediatric Risk, Injury, Failure, Loss, End-Stage Renal Disease score on the clinical course of PICU patients. Pediatr Crit Care Med 16:e275–e282
Piepsz A, Tondeur M, Ham H (2006) Revisiting normal (51)Cr-ethylenediaminetetraacetic acid clearance values in children. Eur J Nucl Med Mol Imaging 33:1477–1482
Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL (2009) New equations to estimate GFR in children with CKD. J Am Soc Nephrol 20:629–637
Hoste L, Dubourg L, Selistre L, De Souza VC, Ranchin B, Hadj-Aissa A, Cochat P, Martens F, Pottel H (2014) A new equation to estimate the glomerular filtration rate in children, adolescents and young adults. Nephrol Dial Transplant 29:1082–1091
Pottel H, Hoste L, Martens F (2012) A simple height-independent equation for estimating glomerular filtration rate in children. Pediatr Nephrol 27:973–979
Rink N, Zappitelli M (2015) Estimation of glomerular filtration rate with and without height: effect of age and renal function level. Pediatr Nephrol 30:1327–1336
Pollack MM, Ruttimann UE, Getson PR (1988) Pediatric risk of mortality (PRISM) score. Crit Care Med 16:1110–1116
Schwartz GJ, Work DF (2009) Measurement and estimation of GFR in children and adolescents. Clin J Am Soc Nephrol 4:1832–1843
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1:307–310
Bernardi MH, Schmidlin D, Ristl R, Heitzinger C, Schiferer A, Neugebauer T, Wrba T, Hiesmayr M, Druml W, Lassnigg A (2016) Serum creatinine back-estimation in cardiac surgery patients: Misclassification of AKI using existing formulae and a data-driven model. Clin J Am Soc Nephrol 11:395–404
Acknowledgements
We acknowledge the research assistants at Centre Hospitalier Universitaire Sainte-Justine, Mariana Dumitrascu, Kahina Bensaadi, and Aldric Desavelle, who performed the data collection and G.M. who performed the validation of the database. We also acknowledge the research assistants at the Montreal Children’s Hospital, Shari Segal, R.A., N.R. who performed data collection, and Jillian Caldwell and M.P. who performed the validation of the database. M.Z. received research support from Fonds de Recherche en Santé du Québec, which allowed him to perform this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics board approval was obtained at both centers. Requirement for patient consent was waived.
Funding
All phases of this study were supported by Fond de recherche du Québec—Santé (FRQS; grant number 22888 [to P.J., J.L., V.P., M.Z.]). M.Z. was also supported by a research salary award and E.H. by a graduate studies award from the FRQS. The authors have no financial conflicts of interest relevant to this article to disclose.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Electronic supplementary material
ESM 1
(DOCX 16 kb)
Rights and permissions
About this article

Cite this article
Hessey, E., Ali, R., Dorais, M. et al. Evaluation of height-dependent and height-independent methods of estimating baseline serum creatinine in critically ill children. Pediatr Nephrol 32, 1953–1962 (2017). https://doi.org/10.1007/s00467-017-3670-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-017-3670-z