
Abstract
Background: There is still some controversy over the need for antireflux procedures with Heller myotomy in the treatment of achalasia. This study was undertaken in an effort to clarify this question.
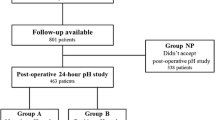
Methods: To determine whether Heller myotomy alone would cause significant gastroesophageal reflux (GER), we studied 16 patients who had undergone laparoscopic Heller myotomy without concomitant antireflux procedures. Patients were asked to return for esophageal manometry and 24-h pH studies after giving informed consent for the Institutional Review Board (IRB)-approved study at a median follow-up time of 8.3 months (range, 3–51). Results are expressed as the mean ± SEM.
Results: Fourteen of the 16 patients reported good to excellent relief of dysphagia after myotomy. They were subsequently studied with a 24-h pH probe and esophageal manometry. These 14 patients had a significant fall in lower esophageal sphincter (LES) pressure from 41.4 ± 4.2 mmHg to 14.2 ± 1.3 mmHg, after the myotomy (p < 0.01, Student's t-test). The two patients who reported more dysphagia postoperatively had LES pressures of 20 and 25 mmHg, respectively. Two of 14 patients had DeMeester scores of >22 (scores = 61.8, 29.4), while only one patient had a pathologic total time of reflux (percent time of reflux, 8%). The mean percent time of reflux in the other 13 patients was 1.9 ± 0.6% (range, 0.1–4%), and the mean DeMeester score was 11.7 ± 4.6 (range, 0.48–19.7).
Conclusions: Laparoscopic Heller myotomy is effective for the relief of dysphagia in achalasia if the myotomy lowers the LES pressure to <17 mmHg. If performed without dissection of the entire esophagus, the laparoscopic Heller myotomy does not create significant GER in the postoperative period. Clearance of acid refluxate from the aperistaltic esophagus is an important component of the pathologic gastroesophageal reflux disease (GERD) seen after Heller myotomy for achalasia. Furthermore, GERD symptoms do not correlate with objective measurement of GE reflux in patients with achalasia. Objective measurement of GERD with 24 h pH probes may be indicated to identify those patients with pathologic acid reflux who need additional medical treatment.
Similar content being viewed by others

Author information
Authors and Affiliations
Additional information
Received: 12 May 1998/Accepted: 15 December 1998
Rights and permissions
About this article
Cite this article
Richards, W., Clements, R., Wang, P. et al. Prevalence of gastroesophageal reflux after laparoscopic Heller myotomy. Surg Endosc 13, 1010–1014 (1999). https://doi.org/10.1007/s004649901158
Published:
Issue Date:
DOI: https://doi.org/10.1007/s004649901158