
Abstract
Background and aim
The risk of lymph node metastasis of a small rectal carcinoid tumor (<10 mm) is known to be lower than that of tumors at other gastrointestinal sites. Although rectal carcinoid tumors can be treated by endoscopic resection, the resected specimen may be incomplete. The consequences of an incomplete resection are not well known.
Method
From December 2008 to November 2015, cases of rectal carcinoid tumors resected by endoscopic resection techniques such as endoscopic submucosal dissection (ESD), or endoscopic mucosal resection using band ligation device (EMR-L), or cap aspiration (EMR-C) were enrolled. The factors associated with incomplete endoscopic resection and clinical outcomes were retrospectively analyzed.
Results
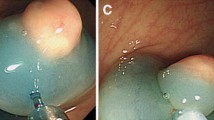
During the study period, a total of 134 rectal carcinoid tumors were resected by endoscopic techniques; ESD (n = 53), EMR-C (n = 65), and EMR-L (n = 16). The mean tumor size was 5.5 ± 2.4 mm. The mean follow-up period was 835 ± 501 days. The en bloc resection and complete resection rates were 100 and 85.8%, respectively. Procedure time was longer and the size of the resected tumor was larger in the ESD group than in the EMR-C or EMR-L (p < 0.001) group by the univariate analysis. A factor related to incomplete resection was central depression on the surface (OR 11.529, 95% CI 2.377–55.922, p = 0.002), as revealed by the multivariate analysis. Nineteen patients had an incomplete resection status and did not undergo additional resection treatment; none of these patients had recurrence during the study period.
Conclusions
A rectal carcinoid tumor with a central depression on the surface was associated with a higher incomplete resection rate. After an incomplete resection of small rectal carcinoid tumors, without evidence of lymphovascular invasion, a periodic follow-up examination without additional resection may be recommended.

Similar content being viewed by others


References
Zhong DD, Shao LM, Cai JT (2013) Endoscopic mucosal resection vs endoscopic submucosal dissection for rectal carcinoid tumours: a systematic review and meta-analysis. Colorectal Dis 15:283–291
Flejou JF (2011) WHO Classification of digestive tumors: the fourth edition. Ann Pathol 31:S27–S31
Maggard MA, O’Connell JB, Ko CY (2004) Updated population-based review of carcinoid tumors. Ann Surg 240:117–122
Jetmore AB, Ray JE, Gathright JB Jr, McMullen KM, Hicks TC, Timmcke AE (1992) Rectal carcinoids: the most frequent carcinoid tumor. Dis Colon Rectum 35:717–725
Konishi T, Watanabe T, Kishimoto J, Kotake K, Muto T, Nagawa H, Japanese Society for Cancer of the C, Rectum (2007) Prognosis and risk factors of metastasis in colorectal carcinoids: results of a nationwide registry over 15 years. Gut 56: 863–868
Soga J (2005) Early-stage carcinoids of the gastrointestinal tract: an analysis of 1914 reported cases. Cancer 103:1587–1595
Park HW, Byeon JS, Park YS, Yang DH, Yoon SM, Kim KJ, Ye BD, Myung SJ, Yang SK, Kim JH (2010) Endoscopic submucosal dissection for treatment of rectal carcinoid tumors. Gastrointest Endosc 72:143–149
Choi CW, Kang DH, Kim HW, Park SB, Jo WS, Song GA, Cho M (2013) Comparison of endoscopic resection therapies for rectal carcinoid tumor: endoscopic submucosal dissection versus endoscopic mucosal resection using band ligation. J Clin Gastroenterol 47:432–436
Park SB, Kim HW, Kang DH, Choi CW, Kim SJ, Nam HS (2015) Advantage of endoscopic mucosal resection with a cap for rectal neuroendocrine tumors. World J Gastroenterol 21:9387–9393
Ramage JK, Ahmed A, Ardill J, Bax N, Breen DJ, Caplin ME, Corrie P, Davar J, Davies AH, Lewington V, Meyer T, Newell-Price J, Poston G, Reed N, Rockall A, Steward W, Thakker RV, Toubanakis C, Valle J, Verbeke C, Grossman AB, Uk, Ireland Neuroendocrine Tumour S (2012) Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours (NETs). Gut 61:6–32
Ono A, Fujii T, Saito Y, Matsuda T, Lee DT, Gotoda T, Saito D (2003) Endoscopic submucosal resection of rectal carcinoid tumors with a ligation device. Gastrointest Endosc 57:583–587
Nagai T, Torishima R, Nakashima H, Ookawara H, Uchida A, Kai S, Sato R, Murakami K, Fujioka T (2004) Saline-assisted endoscopic resection of rectal carcinoids: cap aspiration method versus simple snare resection. Endoscopy 36:202–205
Hyun JH, Lee SD, Youk EG, Lee JB, Lee EJ, Chang HJ, Sohn DK (2015) Clinical impact of a typical endoscopic features in rectal neuroendocrine tumors. World J Gastroenterol 21:13302–13308
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Disclosures
Cheol Woong Choi, Su Bum Park, Dae Hwan Kang, Hyung Wook Kim, Su Jin Kim, Hyeong Seok Nam, and Dae Gon Ryu have no conflicts of interest or financial ties to declare.
Additional information
Hyung Wook Kim and Dae Hwan Kang have contributed equally to this work and are co-correspondences for this article.
Rights and permissions
About this article

Cite this article
Choi, C.W., Park, S.B., Kang, D.H. et al. The clinical outcomes and risk factors associated with incomplete endoscopic resection of rectal carcinoid tumor. Surg Endosc 31, 5006–5011 (2017). https://doi.org/10.1007/s00464-017-5497-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-017-5497-x