
Abstract
Background
The robotic platform might offer superior ergonomics over other minimally invasive approaches. However, the increased time required for instrument set-up, operations, and surgical training are perceived as major drawbacks. There is limited literature on this topic, therefore we report our experience at an academic tertiary medical center in the USA. The primary aim of this study was to analyze the learning curve and the times for necessary steps for singly docked totally robotic Roux-en-Y gastric bypass (RREYGB).
Materials and methods
From November 2010 to April 2013, all consecutive patients who underwent RREYGB were retrospectively analyzed from a prospectively maintained database. Variables of interest for this study were patient demographics, preoperative body mass index, previous surgical history, clinically relevant perioperative events, and operative times for various steps in the procedure.
Results
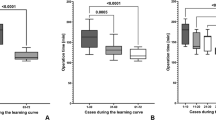
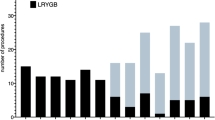
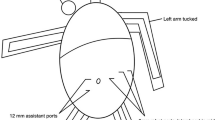
During the study period, a total of 32 patients were enrolled. The mean age was 39.9 ± 9.7 years (range 25–60), preoperative weight was 120.9 ± 21.5 kg (range 76.7–184.6), and body mass index (BMI) was 44.7 ± 5.3 kg/m2 (range 36.1–61). The mean total operative time was 187.3 ± 36.4 min (range 130–261). The time necessary for trocar placement was 11.9 ± 4.5 min (range 4–23), robot set-up was 8.5 ± 3.6 min (range 3–20), pouch creation was 32 ± 10.11 min (range 16–56), gastrojejunal anastomosis was 59.5 ± 12.3 min (range 39–90), jejunojejunal anastomosis was 33.5 ± 9.6 min (range 18–65), and endoscopy/hemostasis was 12.9 ± 7.2 min (range 2–34). Operative time significantly improved after eight cases.
Conclusion
In a high-volume established robotic bariatric center, robot set-up, operative times, and learning curve are shorter than previously reported.


Similar content being viewed by others
References
Selber JC, Baumann DP, Holsinger FC (2012) Robotic latissimus dorsi muscle harvest: a case series. Plast Reconstr Surg 129:1305–1312
Bonatti J, Wehman B, de Biasi AR, Jeudy J, Griffith B, Lehr EJ (2012) Totally endoscopic quadruple coronary artery bypass grafting is feasible using robotic technology. Ann Thorac Surg 93:e111–e112
Boggi U, Signori S, Vistoli F, D’Imporzano S, Amorese G, Consani G, Guarracino F, Marchetti P, Focosi D, Mosca F (2012) Laparoscopic robot-assisted pancreas transplantation: first world experience. Transplantation 93:201–206
Intuitive Surgical, Inc. Q4 2012 Earnings Call Transcript. Available from: http://www.morningstar.com/earnings/earnings-call-transcript.aspx?t=ISRG. Accessed 19 Mar 2013
Breitenstein S, Nocito A, Puhan M, Held U, Weber M, Clavien PA (2008) Robotic-assisted versus laparoscopic cholecystectomy: outcome and cost analyses of a case-matched control study. Ann Surg 247:987–993
De Ugarte DA, Etzioni DA, Gracia C, Atkinson JB (2003) Robotic surgery and resident training. Surg Endosc 17:960–963
Musch M, Roggenbuck U, Klevecka V, Loewen H, Janowski M, Davoudi Y, Kroepfl D (2013) Does changeover by an experienced open prostatic surgeon from open retropubic to robot-assisted laparoscopic prostatectomy mean a step forward or backward? ISRN Oncol 2013:768647
Tyler JA, Fox JP, Desai MM, Perry WB, Glasgow SC (2013) Outcomes and costs associated with robotic colectomy in the minimally invasive era. Dis Colon Rectum 56:458–466
Paraiso MF, Ridgeway B, Park AJ, Jelovsek JE, Barber MD, Falcone T, Einarsson JI (2013) A randomized trial comparing conventional and robotically assisted total laparoscopic hysterectomy. Am J Obstet Gynecol. doi:10.1016/j.ajog.2013.02.008
Lasser MS, Patel CK, Elsamra SE, Renzulli JF 2nd, Haleblian GE, Pareek G (2012) Dedicated robotics team reduces pre-surgical preparation time. Indian J Urol 28:263–266
Gastrointestinal Surgery for Severe Obesity1991. NIH Consensus Statement, 9:1–20
Heemskerk J, van Dam R, van Gemert WG, Beets GL, Greve JW, Jacobs MJ, Bouvy ND (2005) First results after introduction of the four-armed da Vinci Surgical System in fully robotic laparoscopic cholecystectomy. Dig Surg 22:426–431
Ruurda JP, Visser PL, Broeders IA (2003) Analysis of procedure time in robot-assisted surgery: comparative study in laparoscopic cholecystectomy. Comput Aided Surg 8:24–29
Delaney CP, Lynch AC, Senagore AJ, Fazio VW (2003) Comparison of robotically performed and traditional laparoscopic colorectal surgery. Dis Colon Rectum 46:1633–1639
Lehnert M, Richter B, Beyer PA, Heller K (2006) A prospective study comparing operative time in conventional laparoscopic and robotically assisted Thal semifundoplication in children. J Pediatr Surg 41:1392–1396
Iranmanesh P, Morel P, Wagner OJ, Inan I, Pugin F, Hagen ME (2010) Set-up and docking of the da Vinci Surgical System: prospective analysis of initial experience. Int J Med Robot 6:57–60
Buchs NC, Pugin F, Bucher P, Hagen ME, Chassot G, Koutny-Fong P, Morel P (2012) Learning curve for robot-assisted Roux-en-Y gastric bypass. Surg Endosc 26:1116–1121
Schauer P, Ikramuddin S, Hamad G, Gourash W (2003) The learning curve for laparoscopic Roux-en-Y gastric bypass is 100 cases. Surg Endosc 17:212–215
Disclosure
Subhashini Ayloo, Eduardo Fernandes, and Nabajit Choudhury have no financial ties or conflicts of interest to be disclosed with regard to this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ayloo, S., Fernandes, E. & Choudhury, N. Learning curve and robot set-up/operative times in singly docked totally robotic Roux-en-Y Gastric bypass. Surg Endosc 28, 1629–1633 (2014). https://doi.org/10.1007/s00464-013-3362-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-3362-0