
Abstract
Background
This study was designed to compare the surgical outcomes of standard and reverse laparoscopic techniques for the treatment of rectovaginal endometriosis.
Methods
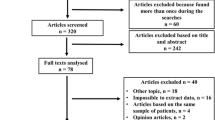
A retrospective study was conducted in a teaching and research hospital (tertiary center), which included 75 women subjected to laparoscopic treatment of rectovaginal endometriosis that required both vaginal resection and rectal surgery. Standard and reverse laparoscopic techniques were compared in 35 and 40 women, respectively. Student’s t test, Mann–Whitney test, and Fisher’s exact test were performed to compare groups when needed; p < 0.05 was considered statistically significant.
Results
There was no statistically significant difference in operating time, blood loss, conversion rate, major intraoperative complications, length of hospital stay, and minor postoperative complications between the two techniques. The rate of major postoperative complications for the standard technique was 22.9%, whereas only 5% for the reverse technique (p = 0.02). The rate of postoperative rectovaginal fistula was the same for both techniques.
Conclusions
Major postoperative complications were reduced by using the reverse technique.


Similar content being viewed by others


References
Carmona F, Martínez-Zamora A, González X, Ginés A, Buñesch L, Balasch J (2009) Does the learning curve of conservative laparoscopic surgery in women with rectovaginal endometriosis impair the recurrence rate? Fertil Steril 92:868–875
Kristensen J, Kjer JJ (2007) Laparoscopic laser resection of rectovaginal pouch and rectovaginal septum endometriosis: the impact on pelvic pain and quality of life. Acta Obstet Gynecol Scand 86:1467–1471
Vercellini P, Crosignani PG, Somigliana E, Berlanda N, Barbara G, Fedele L (2009) Medical treatment for rectovaginal endometriosis: what is the evidence? Hum Reprod 24:2504–2514
Slack A, Child T, Lindsey I, Kennedy S, Cunningham C, Mortensen N, Koninckx P, McVeigh E (2007) Urological and colorectal complications following surgery for rectovaginal endometriosis. BJOG 114:1278–1282
Maytham G, Dowson H, Levy B, Kent A, Rockall T (2010) Laparoscopic excision of rectovaginal endometriosis: report of a prospective study and review of the literature. Colorectal Dis 12(11):1105–1112
Matsuzaki S, Houlle C, Botchorishvili R, Pouly JL, Mage G, Canis M (2009) Excision of the posterior vaginal fornix is necessary to ensure complete resection of rectovaginal endometriotic nodules of more than 2 cm in size. Fertil Steril 91:1314–1315
Darai E, Thomassin I, Barranger E, Detchev R, Cortez A, Houry S, Bazot M (2005) Feasibility and clinical outcome of laparoscopic colorectal resection for endometriosis. Am J Obstet Gynecol 192:394–400
Darai E, Ackerman G, Bazot M, Rouzier R, Dubernard G (2007) Laparoscopic segmental colorectal resection for endometriosis: limits and complications. Surg Endosc 21:1572–1577
Benbara A, Fortin A, Martin B, Palazzo L, Le Tohic A, Madelenat P, Yazbeck C (2008) Surgical and functional results of rectosigmoidal resection for severe endometriosis. Gynecol Obstet Fertil 36:1191–1201
Ferrero S, Anserini P, Abbamonte LH, Ragni N, Camerini G, Remorgida V (2009) Fertility after bowel resection for endometriosis. Fertil Steril 92:41–46
Mohr C, Nezhat FR, Nezhat CH, Seidman DS, Nezhat CR (2005) Fertility considerations in laparoscopic treatment of infiltrative bowel endometriosis. JSLS 9:16–24
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Cornillie FJ, Oosterlynck D, Lauweryns JM, Koninckx PR (1990) Deeply infiltrating pelvic endometriosis: histology and clinical significance. Fertil Steril 53:978–983
Koninckx PR, Martin DC (1992) Deep endometriosis: a consequence of infiltration or retraction or possibly adenomyosis externa? Fertil Steril 58:924–928
Vercellini P, Frontino G, Pietropaolo G, Gattei U, Daguati R, Crosignani PG (2004) Deep endometriosis: definition, pathogenesis, and clinical management. J Am Assoc Gynecol Laparosc 11:153–161
Wright JT (2000) The diagnosis and management of infiltrating nodular recto-vaginal endometriosis. Curr Opin Obstet Gynecol 12:283–287
Kwok A, Lam A, Ford R (2001) Deeply infiltrating endometriosis: implications, diagnosis, and management. Obstet Gynecol Surv 56:168–177
Jacobson TZ, Barlow DH, Garry R, Koninckx P (2001) Laparoscopic surgery for pelvic pain associated with endometriosis. Cochrane Database Syst Rev 4:CD001300
Chapron C, Jacob S, Dubuisson JB, Vieira M, Liaras E, Fauconnier A (2001) Laparoscopically assisted vaginal management of deep endometriosis infiltrating the rectovaginal septum. Acta Obstet Gynecol Scand 80:349–354
Mangler M, Loddenkemper C, Lanowska M, Bartley J, Schneider A, Köhler C (2008) Histopathology-based combined surgical approach to rectovaginal endometriosis. Int J Gynaecol Obstet 103:59–64
Ruffo G, Scopelliti F, Scioscia M, Ceccaroni M, Mainardi P, Minelli L (2010) Laparoscopic colorectal resection for deep infiltrating endometriosis: analysis of 436 cases. Surg Endosc 24:63–67
Koh CH, Janik GM (2002) The surgical management of deep rectovaginal endometriosis. Curr Opin Obstet Gynecol 14:357–364
Redwine DB (1991) Conservative laparoscopic excision of endometriosis by sharp dissection: life table analysis of reoperation and persistent or recurrent disease. Fertil Steril 56:628–634
Fedele L, Bianchi S, Zanconato G, Bettoni G, Gotsch F (2004) Long-term follow-up after conservative surgery for rectovaginal endometriosis. Am J Obstet Gynecol 190:1020–1024
Ford J, English J, Miles WA, Giannopoulos T (2004) Pain, quality of life and complications following the radical resection of rectovaginal endometriosis. BJOG 111:353–356
Burke P, Mealy K, Gillen P, Joyce W, Traynor O, Hyland J (1994) Requirement for bowel preparation in colorectal surgery. Br J Surg 81:907–910
Miettinen RP, Laitinen ST, Mäkelä JT, Pääkkönen ME (2000) Bowel preparation with oral polyethylene glycol electrolyte solution vs. no preparation in elective open colorectal surgery: prospective, randomized study. Dis Colon Rectum 43:669–675
Muzii L, Angioli R, Zullo MA, Calcagno M, Panici PB (2003) Bowel preparation for gynecological surgery. Crit Rev Oncol Hematol 48:311–315
Santos JC Jr, Batista J, Sirimarco MT, Guimarães AS, Levy CE (1994) Prospective randomized trial of mechanical bowel preparation in patients undergoing elective colorectal surgery. Br J Surg 81:1673–1676
Platell C, Hall J (1998) What is the role of mechanical bowel preparation in patients undergoing colorectal surgery? Dis Colon Rectum 41:875–882
Possover M, Diebolder H, Plaul K, Schneider A (2000) Laparoscopically assisted vaginal resection of rectovaginal endometriosis. Obstet Gynecol 96:304–307
Hollett-Caines J, Vilos GA, Penava DA (2003) Laparoscopic mobilization of the rectosigmoid and excision of the obliterated cul-de-sac. J Am Assoc Gynecol Laparosc 10:190–194
Disclosures
William Kondo, Nicolas Bourdel, Kris Jardon, Stefano Tamburro, Daniele Cavoli, Sachiko Matsuzaki, Revaz Botchorishvili, Benoit Rabischong, Jean L. Pouly, Gérard Mage, Michel Canis have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kondo, W., Bourdel, N., Jardon, K. et al. Comparison between standard and reverse laparoscopic techniques for rectovaginal endometriosis. Surg Endosc 25, 2711–2717 (2011). https://doi.org/10.1007/s00464-011-1635-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-011-1635-z