
Abstract
Background
Critics of minimally invasive methods sometimes argue that the summed lengths of all trocar sites have a morbidity similar to that for an open incision of equal length. This argument assumes correctly that pain and scarring are proportional to the total tension normal to a linear incision. But the argument also assumes that total tension sums linearly with incision length. This report demonstrates why that premise is not valid.
Methods
Wounds of various sizes are compared using a simple mathematical model. The closing tension perpendicular to any linear incision is a function of the incision’s length, varying symmetrically together with a maximum at the midpoint of length. If tension rises linearly across an incision, integration of the tension relationship demonstrates that the total wound tension actually is proportional to the square of the length. In this report, incisions of various lengths are modeled, and plausible alternative incision scenarios for various procedures (e.g., Nissen, appendectomy) are compared.
Results
Total tension rises nonlinearly with increasing wound length. Thus, total tension across multiple incisions is always less than the total tension for an incision of the same total length. For example, an open appendectomy creates 2.7-fold more wound tension than a laparoscopic appendectomy. Similarly, two 3-mm trocars create less total tension than a single 5-mm trocar.
Conclusion
Conventional incisions are subject to more total tension than any combination of trocar incisions of equal total length. This inequality yields three clinically relevant corollaries. First, it supports the practice of using the smallest effective trocars (or even no-trocar methods) to minimize pain and scar. Second, addition of a trocar in difficult cases adds relatively little morbidity. Finally, using two small trocars is better than using a single larger trocar.


Similar content being viewed by others


References
Morrow SE, Newman KD (2007) Current management of appendicitis. Semin Pediatr Surg 16:34–40
O’Dwyer PJ, Courtney CA (2003) Factors involved in abdominal wall closure and subsequent incisional hernia. Surgeon 1:17–22
Pietramaggiori G et al (2007) Tensile forces stimulate vascular remodeling and epidermal cell proliferation in living skin. Ann Surg 246:896–902
Bhadal N et al (2008) The effect of mechanical strain on protease production by keratinocytes. Br J Dermatol 158:396–398
Akaishi S, Akimoto M, Ogawa R, Hyakusoku H (2008) The relationship between keloid growth pattern and stretching tension: visual analysis using the finite element method. Ann Plast Surg 60:445–451
Scott NW et al (2002) Open mesh versus nonmesh for repair of femoral and inguinal hernia. Cochrane Database Syst Rev (4):CD002197
Kurzer M, Belsham PA, Kark AE (2004) Tension-free mesh repair of umbilical hernia as a day case using local anaesthesia. Hernia 8:104–107
Marwah S, Marwah N, Singh M, Kapoor A, Karwasra RK (2005) Addition of rectus sheath relaxation incisions to emergency midline laparotomy for peritonitis to prevent fascial dehiscence. World J Surg 29:235–239
Retel V et al (2001) Nonlinear model of skin mechanical behaviour analysis with finite element method. Skin Res Technol 7:152–158
Lott-Crumpler DA, Chaudhry HR (2001) Optimal patterns for suturing wounds of complex shapes to foster healing. J Biomech 34:51–58
Mathias JM (1997) Needlescopic surgery is painless and scarless. OR Manager 13(24):26–27
Bisgaard T, Klarskov B, Trap R, Kehlet H, Rosenberg J (2002) Microlaparoscopic vs conventional laparoscopic cholecystectomy: a prospective randomized double-blind trial. Surg Endosc 16:458–464
Canes D et al (2008) Transumbilical single-port surgery: evolution and current status. Eur Urol 54:1020–1029
Rescorla FJ, West KW, Engum SA, Grosfeld JL (2007) Laparoscopic splenic procedures in children: experience in 231 children. Ann Surg 246:683–687 discussion 687–688
Weisstein EW (2003) CRC concise encyclopedia of mathematics, 2nd edn. Chapman & Hall/CRC, Boca Raton, p 3242
Disclosures
Thane Blinman has no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Box 1
How long is a trocar incision? Most trainees, when asked how long to make an incision for trocar placement, underestimate the incision length required. For instance, when asked how long to make an incision for a 5-mm trocar, most answer, surprisingly, “4 mm.” However, a little geometry shows the correct answer. First, it is assumed that skin is inelastic. Second, it is assumed that a trocar has an outer diameter of 5 mm (most commercial trocars actually have an outer diameter slightly greater than 6 mm). To create a linear incision that produces a circular aperture large enough for the trocar, it is plain that the incision needs to be one-half of the circumference of that circle:

A trocar with an outer diameter of 5 mm therefore requires an incision length of approximately 3.14 × 5/2 = 7.85 mm. Why does this matter? If the surgeon makes the incision too short, dangerous force may be required to place the trocar as the skin is forced open around the trocar shaft, leading to injury of the organs below. Then, the extra shear also will crush skin edges, leading to ugly closures more prone to failure and infection. Conversely, incisions that are too large will leave the trocars too loose. Consequently, they may slide in and out of the abdominal wall during the case, leading to decreased precision and delays as the trocars are constantly repositioned. On the other hand, understanding this geometry allows the surgeon to make correctly sized incisions for trocars of any size.
Box 2
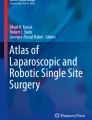
What about “single-port” laparoscopy? Single-port laparoscopy is advocated by those who assume that one single port, of whatever size, is less morbid than three trocars positioned in the abdomen for maximal mechanical advantage. Is this true? Assume that a given operation can be done with either three 5-mm ports or one single aperture that contains all three 5-mm ports. How large must the diameter of the aperture be to accommodate all three ports? We can calculate the inner diameter, R 3, required to contain most efficiently three circular ports of given radius, R 1:

From the figure, it is apparent that the minimal inner diameter, R 3, required for a trocar of an outer diameter, R 1, is the sum:
where R 2 is the radius of the circle circumscribing a triangle connecting the centers of the three trocar circles [15]:
where a is the length of the triangle. But because a = 2 × R 1, R 2 is: Thus the inner radius of the circle R 3 is:
This means that the inner radius of a circle required for three 5-mm trocars is roughly 5.4 mm, or a diameter of 10.8 mm. From Box 1, we see that this requires an incision of 10.8 × π/2, or approximately 16.6 mm. The relative tension of a 16.6-mm incision versus three 7.85-mm incisions is approximately a 1.5-fold increase. In other words, it can be expected that, at best, single-port laparoscopy produces an incision adding about 50% of the tension required by three conventionally-positioned trocars.