
Abstract
Due to potential lethality of healthcare-associated sepsis (HAS), a low threshold for blood culturing and antimicrobial therapy (ABT) initiation is accepted. We assessed variability in the trigger for blood culturing between three neonatal intensive care units. A multicenter prospective cohort study was conducted. In newborns with suspicion of HAS, 10 predefined clinical signs, nosocomial sepsis (NOSEP) score, C-reactive protein, ABT initiation, and risk factors were registered at time of culturing. Outcome was lab-confirmed HAS, defined according to the NeoKISS-criteria. Two hundred ninety-nine suspected HAS episodes were considered in 212 infants, of which 118 had birth-weight ≤ 1500 g; proportion of lab-confirmed HAS per suspected episode was 30/192 (center 1), 28/60 (center 2), and 8/47 (center 3) (p < 0.001). Median C-reactive protein and number of clinical signs at time of culturing differed between centers 1, 2, and 3 (respectively 11 vs. 5 vs. 3 mg/L, p = 0.001; 1 sign [IQR 0–2, center 1] vs. 3 signs [IQR 2–4, centers 2 and 3], p < 0.001). Median NOSEP score at time of culturing was 5 (IQR 3–8, center 1), 5 (IQR 3–9, center 2), and 8 (IQR 5–11, center 3) (p = 0.016). Difference in ABT initiation was noticed (82 vs. 93 vs. 74%, p = 0.05).
Conclusion: Center heterogeneity in sampling practice is substantial. Optimizing sampling practice can be recommended.
What is Known: | |
• Blood culture test is a common diagnostic procedure in critically-ill newborns. • A low threshold for sampling and antimicrobial therapy initiation is accepted. | |
What is New: • Variability in blood culture practice was assessed between 3 neonatal intensive care units by the registration of sampling frequencies, clinical indications, and antimicrobial therapy initiation. |
Similar content being viewed by others

Introduction
Healthcare-associated sepsis (HAS) is the most frequent infectious complication in neonatal intensive care units (NICUs) with substantial risk for neurological sequelae and mortality [13, 28, 30, 31, 33]. The blood culture is the gold standard for sepsis diagnosis and is one of the most commonly executed diagnostic procedure in infants admitted to a NICU. The majority of the cultures are sampled on the day of birth and approximately 40% are sampled in suspicion of HAS [4]. Guidelines on clinical indications for blood culturing in neonates suspected for HAS are lacking so various thresholds for sampling are assumed. Moreover, due to the potential severity and lethality of HAS, a low threshold for sampling and antimicrobial therapy (ABT) initiation is accepted [32]. In addition, blood culturing is time-consuming and imprecise so early and correct diagnosis of HAS is challenging and mostly based on judgment of clinical signs and inflammatory biomarkers [6, 25, 26]. Much attention is for the predictive value of biomarkers such as C-reactive protein (CRP), procalcitonin, and anti-inflammatory cytokines. However, those biomarkers can be of noninfectious origin and may not have the ability to differentiate between several inflammation sources [2, 21, 22, 37]. Likewise for individual clinical signs which are mostly subtle and difficult to interpret, predictive value is questionable [34].
We hypothesize that blood culture sampling practice differs between NICUs because of the lack of guidelines. For this, our objective is to describe blood culture sampling frequencies, clinical indications for sampling, and ABT administration in three NICUs.
Methods
Study design and population
We performed a multicenter prospective cohort study. All neonates admitted to the NICU of three Belgian tertiary referral hospitals for ≥ 48 h were eligible for inclusion. During an 18-month study period (July 2013–December 2014), a consecutive series of blood cultures obtained as part of a sepsis evaluation were included; cultures sampled within 7 days of each other and after ABT initiation were excluded. The outcome of a suspected episode was classified in “lab-confirmed sepsis,” “clinical sepsis,” or “no sepsis.” Classification was made by the principal investigator (E.V.).
Center 1 and center 2 are academic hospitals with respectively a 32-bed and 28-bed NICU; center 3 is a non-academic hospital with a 32-bed NICU. The yearly mean NICU admission rate of center 1 is approximately 550 of which circa 18% are very low birth-weight (VLBW) neonates (≤ 1500 g); specialist services include pediatric cardiology and cardiac surgery. For centers 2 and 3, the yearly NICU admission rate is approximately 400 and 470 respectively of which 25 and 15% are VLBW. Only newborns (i.e., less than 28 days of life) are admitted to these units.
Sampling practice: data collection
Prospective registration of nosocomial sepsis (NOSEP) score [17] (including CRP ≥ 14 mg/L, neutrophil fraction > 50%, temperature > 38.2 °C, total parenteral nutrition [TPN] ≥ 14 days, thrombocytopenia < 150 × 103/μL), 10 predefined clinical signs [19] (including increased/acute onset of tachypnea/oxygen need, apnea/bradycardia, hypotension, glucose intolerance, impaired peripheral perfusion, lethargy, temperature instability, ileus or feeding intolerance, oliguria, base deficit), CRP value, and ABT initiation were completed at time of sampling by the attending neonatologist using sticker labels; assessment of clinical signs encompasses an interpretation period of ≤ 24 h preceding sampling. Also, registration of risk factors for HAS was performed (including gender, birth-weight, gestational age, intra-uterine growth restriction, type of catheterization, TPN days, mechanical ventilation for ≥ 24 h prior to culturing, recent major surgery ≤ 7 days prior to culturing, postnatal steroid administration prior to culturing, pathogen, days of antibiotics, other infection, and length of stay). Blood cultures were sampled by venipuncture or from a newly inserted central line; volume was standardized at 1 mL; skin or catheter-hub disinfection time was standardized at 30 s. In center 2, sampling was indicated when a NOSEP score of ≥ 8 was attained. Center 1 and center 3 did not use any protocol or procedure in guidance of sampling. In all centers, blood cultures were assessed using the BacT/Alert 3D automated microbial detection system (bioMérieux Inc., Durham, NC).
Definitions and classification
HAS: occurs ≥ 48 h after birth [15].
Lab-confirmed sepsis: a pathogen is detected in a blood, urine, or cerebrospinal fluid culture or X-ray-confirmed ventilator-associated pneumonia and necrotizing enterocolitis. When the causative pathogen is a skin commensal, mainly coagulase-negative staphylococci, additional criteria are needed: two clinical signs and a CRP of > 20 mg/L [11].
Clinical sepsis: presence of two clinical signs and ABT initiation of ≥ 5 days when no pathogen was detected in one or more cultures and no apparent other site of infection is assumed [11], or a skin commensal was detected plus presence of two clinical signs and ABT initation for 5 days or more and no apparent other site of infection is assumed.
No sepsis: not meeting criteria of clinical sepsis or contamination (skin commensal not meeting criteria for clinical sepsis).
Statistics
Logistic regression was used to determine the association between the indicators and lab-confirmed sepsis (“no sepsis” and “clinical sepsis” as controls); the association of patient-specific risk factors (“birth-weight,” “gestational age,” “gender,” and “intra-uterine growth restriction”) was only evaluated for the first suspected HAS episode. Unadjusted odds ratios (ORs) and 95% confidence intervals (CI) were calculated. The statistical package of social science version 21 was utilized for all tests (SPSS Inc., Chicago, IL).
Ethics committee
The study was approved by the ethics committee of the participating centers.
Results
Patients
A total of 413 blood culture samples in 301 neonates were registered. Of these 413 samples, 95 were excluded because of prior ABT and an additional 19 because of reiteration ≤ 7 days. For final analysis, 299 samples in 212 neonates were included of which 118 (55.7%) had birth-weight ≤ 1500 g; median birth-weight, gestational age, and length of stay were respectively 1363 g (interquartile range [IQR], 919–2165), 31 weeks (IQR 27–35), and 41 days (IQR 20–77). Characteristics of the 212 included neonates are displayed per center in Table 1.
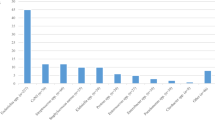
Pathogen distribution of the lab-confirmed episodes is presented in Table 2.
Episode classification and incidence
Classification of the suspected episodes and incidence per center are in Table 3. Among the 299 included samples, respectively 66 (22.1%), 74 (24.7%), and 157 (52.6%) were classified as “lab-confirmed sepsis,” “clinical sepsis,” and “no sepsis.”
The proportion of blood cultures sampled in suspicion of HAS per total admissions during the 18-month study period was respectively 23.3% (center 1, 192/825), 10.0% (center 2, 60/600), and 6.7% (center 3, 47/704) (p < 0.001); the proportion of lab-confirmed + clinical sepsis per suspected episodes was respectively 36% (70/192, center 1), 77% (46/60, center 2), 55% (26/47, center 3) (p < 0.001).
Sampling practice
Differences between centers in sampling practice are presented in Table 4.
For the total cohort, the median number of clinical signs per suspected episodes was significantly lower for the cohort “no sepsis” (1, IQR 0–1) compared to “lab-confirmed sepsis” (3, IQR 1–4) (p < 0.001); in contrast, median CRP was not significantly different between these two cohorts, respectively 10.0 mg/L (IQR 0.0–22.3) for “no sepsis” and 9.0 mg/L (IQR 1.8–27.5) for “lab-confirmed sepsis” (p = 0.81).
Of all suspected episodes with ≥ 5-day ABT administration, respectively 48% (70/146, center 1), 100% (46/46, center 2), and 84% (26/31, center 3) (p < 0.001) were classified as for “lab-confirmed sepsis” or “clinical sepsis.”
Concerning the NOSEP score of 8 as indicator for sampling in center 2, 39 suspected episodes (65%) did not reach this score. The median number of clinical signs at time of culturing of these 39 cases was 2 (IQR 1–4) and the median number of clinical signs of the 21 cases with a NOSEP score of 8 was 3 (IQR 2–4) (p = 0.019).
Association of indicators with lab-confirmed sepsis
Unadjusted odds of clinical indicators and risk factors for lab-confirmed HAS are reported in Table 5.
Discussion
We described sampling practice in suspicion of HAS; substantial differences between the centers were observed. Additionally, bivariate analysis of indicators for lab-confirmed sepsis revealed that most clinical signs were not associated with lab-confirmed sepsis; in contrast, the ad random combination of 2 and 3 clinical signs was associated.
Incidence
Significant difference in incidence between the centers (3.6% center 1, 4.6% center 2, 1.1% center 3) and in the proportion of samples per total admissions (23.3% center 1, 10% center 2, 6.7% center 3) can indicate a case-mix in population and/or variance in sampling practice. Since in center 1 risk profile for HAS seems lower (i.e., higher median birth-weight and gestational age) and proportion of samples per total admission is higher, difference in sampling practice is assumed [7]. To our knowledge, research on sampling frequencies in neonates is limited. Blackburn et al. [4] reported a 48% proportion of samples/admissions in a tertiary neonatal unit in London at “day of birth” of which 15% were lab-confirmed on day 8. Unfortunately, our results are incomparable because of the focus on blood cultures sampled after 48 h of admission.
Sampling practice
For center 1, a proportion of 27% zero clinical signs per suspected episode, a median of 1 clinical sign, and a median CRP of 11 mg/L at time of culturing might indicate a sampling practice based on CRP value or probably other biomarkers or risk factors. Another possible explanation for the high proportion of samples in the absence of clinical signs might be that some doctors perform a systematic weekly sampling in specific cases, although this was not defined as a standard procedure. Contrariwise for the other centers, sampling practice was more driven by clinical signs and not by CRP value. Similar to centers 2 and 3 are the results of Bekhof et al. [3] wherein more than half of their suspected HAS cohort (65%) had normal CRP (i.e., ≤ 10 mg/L). This result is in contrast with the results of Ohlin et al. [23] conducted on 401 neonates with suspected bloodstream infection of which 129 were in suspicion of HAS; they found that only 22% had a CRP < 10 mg/L.
Remarkable are the results for center 2. The highest proportion of lab-confirmed + clinical sepsis per suspected episode was observed (77 vs. 36% center 1 and 55% center 3) potentially indicating a more efficient sampling practice. Since the scope of this study was solely a description of sampling practice features, we did not assess the clinical consequences for the neonate. For this, we cannot judge whether the policy of center 2 is truly more efficient than the policies of the other centers. Furthermore, this center uses a NOSEP score of 8 in guidance of blood culturing; however, only 35% of the suspected episodes had a score of 8 or more, so in 65% of the episodes sampling was executed because of other indication(s). For the 65% not reaching a NOSEP score of 8, a median of two clinical signs at time of culturing was observed, so it is assumed that the presence of two clinical signs could also indicate sampling in this center. We note that episodes with a NOSEP score of 8 had significantly more clinical signs at time of blood culturing than episodes without a NOSEP score of 8; this may implicate an association with NOSEP and the clinical condition of the neonate in suspicion of HAS.
Because of the possible devastating consequences of HAS, a low threshold for initiating ABT is generally accepted [9]. Nonetheless, inadequate, inappropriate empiric treatment can foster antimicrobial resistance, compromise gastrointestinal immunity, and be associated with adverse outcomes [1, 12]. We observed that in all centers, blood cultures were taken without ABT initiation (note that follow-up cultures, as a part of ABT evaluation procedure, are excluded). The rationale for not starting antibiotics might also be that some doctors perform a systematic weekly sampling in specific cases. Implementing antimicrobial stewardship programs can be helpful to reduce antimicrobial initiation and duration in NICU [5, 20, 27, 36].
Association of indicators with lab-confirmed sepsis
Unadjusted regression analysis confirms that most clinical signs are in separation no specific sepsis indicators; only “ileus/feeding intolerance” and “impaired peripheral perfusion” appear to be specific symptoms for lab-confirmed sepsis. Since heterogeneity in symptom definition and population is observed, comparison with other research results is difficult. Modi et al. [19] searched for clinical signs associated with lab-confirmed sepsis in low-gestational-age infants (≤ 31 weeks) and found that all 10 signs, as applied in our study, were significantly associated. Although the same definitions of these signs were used, comparison with Modi et al. [19] is probably inappropriate since they included all NICU patients. As the median number of clinical signs is significantly higher for “lab-confirmed” compared to “no sepsis” and the occurrence of two or three ad random clinical signs at time of culturing have higher odds for “lab-confirmed sepsis,” the presence of several clinical signs can be valuable as sepsis indicator.
We did not find an association between “CRP rise” and “lab-confirmed sepsis” which is in contrast to the study results of Ohlin et al. [23] and Mahieu et al. [17] but in agreement with other studies [16, 29]. The predictive value of CRP is controversial since a CRP rise is known as a late diagnostic marker for infection [10, 16, 29].
“Mechanical ventilation” or “respiratory distress,” “peripheral or central line catheterization,” and impaired peripheral perfusion are well-known risk factors for HAS and frequently included in prediction models [3, 8, 13, 24, 35]. We agree with these well-known individual risk factors and clinical characteristics of infection. Though, according to Mahieu et al.[17] when using multivariate analysis other risk factors such as prolonged exposure to TPN seem more important than the confounding factors “mechanical ventilation” and prolonged exposure to “central line catheterization”. Moreover, at time of the NOSEP score development, only objective clinical characteristics were taken into account to exclude the subjective interpretation by the bedside physician and/or nurse. Therefore, “respiratory distress” and “poor peripheral perfusion” were not taken into account for the development of the NOSEP prediction model.
Prediction of HAS is a major issue in neonatal intensive care; unspecific signs and case-mix hamper the development of accurate prediction models. However, the NOSEP score is perceived with moderate diagnostic accuracy and is externally validated with good AUC after redefining cutoff of NOSEP items [17, 18]. Our observations in clinical practice revealed that a score of 8 as a separate indicator did not seem sufficient in guidance of blood culturing. Additionally, the unadjusted odds of NOSEP score 8, i.e., 1.6 (0.9–2.8), are only borderline significant. In contrast, for center 2, the combination of NOSEP sore 8 and several clinical signs might have led to an efficient sampling practice as stated earlier. For this and because it is our belief that clinically ill neonates cannot be left without initiation of diagnostic procedures and treatment, it may be appropriate to use the presence of two clinical signs as a threshold for blood culturing.
Limitations and recommendations
It is possible that some infants might be wrongly classified since blood culture test is imprecise. However, our applied definition of lab-confirmed sepsis caused by skin commensals with additional criteria most probably exclude the false-positive cultures.
In clinical practice, the interpretation of the non-specific clinical signs is not always obvious and probably facing inter-observer variability which might have influenced our results. Nevertheless, for most clinical signs, standardized definitions were used. Also, limited incidence of some clinical signs might have introduced bias (type I error) in unadjusted regression analysis.
When a larger cohort (including a control group) is obtained, future research can explore the benefit of using prediction models in guidance of sampling practice; assessment of mortality and morbidity directly attributable to HAS can help to judge the different policies. Less blood culture samples result in less workload for the staff, a financial profit for the hospital, and can result in appropriate ABT [14, 36]. Moreover, we cannot ignore the decreased burden for neonate.
Conclusion
Center heterogeneity in sampling practice is substantial. Optimizing sampling practice can be recommended. Although not obvious to uniform due to case-mix in population, guidelines might be helpful and desirable.
Abbreviations
- ABT:
-
Antimicrobial therapy
- CRP:
-
C-reactive protein
- CI:
-
Confidence interval
- HAS:
-
Healthcare-associated sepsis
- IQR:
-
Interquartile range
- NICU:
-
Neonatal intensive care unit
- NOSEP score:
-
Nosocomial sepsis score
- OR:
-
Odds ratio
- TPN:
-
Total parenteral nutrition
- VLBW:
-
Very low birth-weight
References
Apisarnthanarak A, Holzmann-Pazgal G, Hamvas A, Olsen MA, Fraser VJ (2004) Antimicrobial use and the influence of inadequate empiric antimicrobial therapy on the outcomes of nosocomial bloodstream infections in a neonatal intensive care unit. Infect Control Hosp Epidemiol 25:735–741
Auriti C, Fiscarelli E, Ronchetti MP, Argentieri M, Marrocco G, Quondamcarlo A, et al (2012) Procalcitonin in detecting neonatal nosocomial sepsis. Arch Dis Child Fetal Neonatal Ed 97:F368–F370
Bekhof J, Reitsma JB, Kok JH, Van Straaten IH (2013) Clinical signs to identify late-onset sepsis in preterm infants. Eur J Pediatr 172:501–508
Blackburn RM, Muller-Pebody B, Planche T, Johnson A, Hopkins S, Sharland M, et al (2012) Neonatal sepsis—many blood samples, few positive cultures: implications for improving antibiotic prescribing. Arch Dis Child Fetal Neonatal Ed 97:F487–F488
Cantey JB, Wozniak PS, Sánchez PJ (2015) Prospective surveillance of antibiotic use in the neonatal intensive care unit: results from the SCOUT study. Pediatr Infect Dis J 34:267–272
Chiesa C, Panero A, Osborn JF, Simonetti AF, Pacifico L (2004) Diagnosis of neonatal sepsis: a clinical and laboratory challenge. Clin Chem 50:279–287
Da Palma Afonso E, Blot S (2017) Effect of gestational age on the epidemiology of late-onset sepsis in neonatal intensive care units—a review. Expert Review of Anti-infective Ther https://doi.org/10.1080/14787210.2017.1379394
Fanaroff AA, Korones SB, Wright LL, Verter J, Poland RL, Bauer CR, et al (1998) Incidence, presenting features, risk factors and significance of late onset septicemia in very low birth weight infants. The National Institute of Child Health and Human Development Neonatal Research Network Pediatr Infect Dis J 17:593–598
Fischer JE, Ramser M, Altermatt S, Nadal D, Waldvogel K (2000) Rational utilisation of antibiotic treatment in critically ill children. Schweiz Med Wochenschr 130:1564–1571
Fowlie PW, Schmidt B (1998) Diagnostic tests for bacterial infection from birth to 90 days—a systematic review. Arch Dis Child Fetal Neonatal Ed 78:F92–F98
Gastmeier P, Geffers C, Schwab F, Fitzner J, Obladen M, Rüden H (2004) Development of a surveillance system for nosocomial infections: the component for neonatal intensive care units in Germany. J Hosp Infect 57:126–131
Gordon A, Jeffery HE (2005) Antibiotic regimens for suspected late onset sepsis in newborn infants. Cochrane Database Syst Rev 3:CD004501
Gupta N, Crockett DC, Anthony M, Webster DP (2011) Late onset bloodstream infections in a tertiary neonatal intensive care unit. Arch Dis Child Fetal Neonatal Ed 96:F234–F234, F237
Gur I, Markel G, Nave Y, Vainshtein I, Eisenkraft A, Riskin A (2014) A mathematical algorithm for detection of late-onset sepsis in very-low birth weight infants: a preliminary diagnostic test evaluation. Indian Pediatr 51:647–650
Horan TC, Andrus M, Dudeck MA (2008) CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 36:309–332
Laborada G, Rego M, Jain A, Guliano M, Stavola J, Ballabh P, et al (2003) Diagnostic value of cytokines and C-reactive protein in the first 24 hours of neonatal sepsis. Am J Perinatol 20:491–501
Mahieu LM, De Muynck AO, De Dooy JJ, Laroche SM, Van Acker KJ (2000) Prediction of nosocomial sepsis in neonates by means of a computer-weighted bedside scoring system (NOSEP score). Crit Care Med 28:2026–2033
Mahieu LM, De Dooy JJ, Cossey VR, Goossens LL, Vrancken SL, Jespers AY, et al (2002) Internal and external validation of the NOSEP prediction score for nosocomial sepsis in neonates. Crit Care Med 30:1459–1466
Modi N, Dore CJ, Saraswatula A, Richards M, Bamford KB, Coello R, et al (2009) A case definition for national and international neonatal bloodstream infection surveillance. Arch Dis Child Fetal Neonatal Ed 94:F8–12
Muller-Pebody B, Johnson AP, Heath PT, Gilbert RE, Henderson KL, Sharland M, et al (2011) Empirical treatment of neonatal sepsis: are the current guidelines adequate? Arch Dis Child Fetal Neonatal Ed 96:F4–F8
Mussap M, Noto A, Cibecchini F, Fanos V (2013) The importance of biomarkers in neonatology. Semin Fetal Neonatal Med 18:56–64
Ng PC (2004) Diagnostic markers of infection in neonates. Arch Dis Child Fetal Neonatal Ed 89:F229–F235
Ohlin A, Bjorkqvist M, Montgomery SM, Schollin J (2010) Clinical signs and CRP values associated with blood culture results in neonates evaluated for suspected sepsis. Acta Paediatr 99:1635–1640
Okascharoen C, Sirinavin S, Thakkinstian A, Kitayaporn D, Supapanachart S (2005) A bedside prediction-scoring model for late-onset neonatal sepsis. J Perinatol 25:778–783
Pammi M, Flores A, Leeflang M, Versalovic J (2011) Molecular assays in the diagnosis of neonatal sepsis: a systematic review and meta-analysis. Pediatrics 128:e973–e985
Paolucci M, Landini MP, Sambri V (2012) How can the microbiologist help in diagnosing neonatal sepsis? Int J Pediatr 2012:120139
Patel SJ, Saiman L (2012) Principles and strategies of antimicrobial stewardship in the neonatal intensive care unit. Semin Perinatol 36:431–436
Pessoa-Silva CL, Miyasaki CH, de Almeida MF, Kopelman BI, Raggio RL, Wey SB (2001) Neonatal late-onset bloodstream infection: attributable mortality, excess of length of stay and risk factors. Eur J Epidemiol 17:715–720
da Silva O, Ohlsson A (1998) How accurate are leukocyte indices and C-reactive protein for diagnosis of neonatal sepsis? Paediatr Child Health 3:158–159
Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, et al (2002) Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics 110:285–291
Stoll BJ, Hansen NI, Adams-Chapman I, Fanaroff AA, Hintz SR, Vohr B, et al (2004) Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. JAMA 292:2357–2365
Tripathi N, Cotten CM, Smith PB (2012) Antibiotic use and misuse in the neonatal intensive care unit. Clin Perinatol 39:61–68
Verstraete E, Boelens J, De Coen K, Claeys G, Vogelaers D, Vanhaesebrouck P, et al (2014) Healthcare-associated bloodstream infections in a neonatal intensive care unit over a 20-year period (1992-2011): trends in incidence, pathogens, and mortality. Infect Control Hosp Epidemiol 35:511–518
Verstraete EH, Blot K, Mahieu L, Vogelaers D, Blot S (2015) Prediction models for neonatal health care-associated sepsis: a meta-analysis. Pediatrics 135:e1002–e1014
Verstraete EH, De Coen K, Vogelaers D, Blot S (2015) Risk factors for health care-associated sepsis in critically ill neonates stratified by birth-weight. Pediatr Infect Dis J 34:1180–1186
Yang YN, Tseng HI, Yang SN, Lu CC, Chen HL, Chen CJ (2012) A strategy for reduction of antibiotic use in new patients admitted to a neonatal intensive care unit. Pediatr Neonatol 53:245–251
Zeitoun AA, Gad SS, Attia FM, Abu Maziad AS, Bell EF (2010) Evaluation of neutrophilic CD64, interleukin 10 and procalcitonin as diagnostic markers of early- and late-onset neonatal sepsis. Scand J Infect Dis 42:299–305
Acknowledgments
Thank you to Dr. Ellen Deschepper for her biostatistical advice.
Funding
Stijn Blot holds a research mandate of the Special Research Fund at Ghent University.
Author information
Authors and Affiliations
Contributions
Evelien Verstraete conceived and designed the study, contributed to the search of published work, dataacquisition, data analysis, data interpretation, drafted and finalized the report.
Ludo Mahieu contributed to the data acquisition, data analysis, data interpretation and critically revised the report.
James D’Haese contributed to the data acquisition, data analysis, and data interpretation.
Kris De Coen contributed to data interpretation, critically revised the report and made substantialcontributions on the final manuscript.
Jerina Boelens contributed to the data acquisition, data analysis, and data interpretation.
Dirk Vogelaers critically revised the report and made substantial contributions on the final manuscript.
Stijn Blot contributed to the search of published work, data analysis, and critically revised the report.
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of interest
The authors declare that they have no conflicts of interest.
Informed consent
For this type of study, formal consent in not required.
Additional information
Communicated by Patrick Van Reempts
Rights and permissions
About this article

Cite this article
Verstraete, E.H., Mahieu, L., d’Haese, J. et al. Blood culture indications in critically ill neonates: a multicenter prospective cohort study. Eur J Pediatr 177, 1565–1572 (2018). https://doi.org/10.1007/s00431-018-3203-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-018-3203-1