
Abstract
The purpose of this study was to identify the clinical, [18F]-fluorodeoxyglucose positron emission tomography (FDG-PET) and amyloid-PET findings in a large cohort of posterior cortical atrophy (PCA) patients, to examine the neural correlates of the classic features of PCA, and to better understand the features associated with early PCA. We prospectively recruited 25 patients who presented to the Mayo Clinic between March 2013 and August 2014 and met diagnostic criteria for PCA. All patients underwent a standardized set of tests and amyloid imaging with [11C] Pittsburg compound B (PiB). Seventeen (68 %) underwent FDG-PET scanning. We divided the cohort at the median disease duration of 4 years in order to assess clinical and FDG-PET correlates of early PCA (n = 13). The most common clinical features were simultanagnosia (92 %), dysgraphia (68 %), poly-mini-myoclonus (64 %) and oculomotor apraxia (56.5 %). On FDG-PET, hypometabolism was observed bilaterally in the lateral and medial parietal and occipital lobes. Simultanagnosia was associated with hypometabolism in the right occipital lobe and posterior cingulum, optic ataxia with hypometabolism in left occipital lobe, and oculomotor apraxia with hypometabolism in the left parietal lobe and posterior cingulate gyrus. All 25 PCA patients were amyloid positive. Simultanagnosia was the only feature present in 85 % of early PCA patients. The syndrome of PCA is associated with posterior hemisphere hypometabolism and with amyloid deposition. Many of the classic features of PCA show associated focal, but not widespread, areas of involvement of these posterior hemispheric regions. Simultanagnosia appears to be the most common and hence sensitive feature of early PCA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Posterior cortical atrophy (PCA) is a neurodegenerative disorder in which the onset of dementia is characterized by the development of higher order visual deficits [1]. This disease is often accompanied by visuospatial and visuoperceptual impairments, alexia, features of Bálint’s syndrome, Gerstmann’s syndrome and transcortical sensory aphasia, whereas episodic memory is relatively preserved or only mildly impaired [2]. These clinical features differ from those of typical dementia of the Alzheimer’s type (DAT) as they show preservation of memory, insight, and judgment until late in the clinical course, when the clinical features of PCA and DAT overlap [3]. The most frequent pathological findings in PCA are tau neurofibrillary tangles and beta-amyloid neuritic plaques which are characteristic of Alzheimer’s disease [4], although other pathologies have been described in PCA including corticobasal degeneration, diffuse Lewy body disease, and Creutzfeldt-Jakob disease [5–7]; frontotemporal dementia with progranulin mutation has also been reported [8].
The use of functional neuroimaging, using [18F]-fluorodeoxyglucose positron emission tomography (FDG-PET) allows the in vivo assessment of brain metabolism. Previous FDG-PET studies in PCA patients have shown prominent hypometabolism in the occipito-parietal region with variable involvement of the frontal eye fields and the relative sparing of the frontal and medial temporal cortex [9–12]. However, in the majority of such studies there is no information on pathology underlying PCA or information on features occurring early in the disease course. Identifying information about underlying pathology is important since different pathologies could have different clinical associations and hence confound the findings in any such study. Additionally, understanding early PCA could have an impact on prognosis and treatment.
In this study, we assessed for the presence of beta-amyloid deposition on Pittsburgh compound B-PET (PiB-PET) scanning in a large cohort of PCA patients and assessed for clinical and FDG-PET findings. Additionally, we assessed for the anatomic correlates of the classic features of PCA and for features that are present early in the disease course.
Methods
Patient recruitment
We prospectively recruited all consecutive patients who presented to the Department of Neurology, Mayo Clinic, Rochester, Minnesota, between March 1st, 2013 and August 31st, 2014 with a clinical diagnosis of PCA who also fulfilled our research criteria for PCA (see below).
Posterior cortical atrophy was defined according to the core criteria previously suggested [4, 13] as follows: (1) insidious onset and gradual progression, (2) presentation of visual complaints in the absence of significant primary ocular disease explaining the symptoms, (3) relative preservation of anterograde memory and insight early in the disorder, (4) disabling visual impairment throughout the disorder, and (5) presence of any of the following: simultanagnosia with or without optic ataxia or oculomotor apraxia, constructional dyspraxia, visual field defect, environmental disorientation or any elements of Gerstmann’s syndrome (acalculia, agraphia, left–right disorientation and finger agnosia).
Patients were included in this study if they also met the following five research criterion for PCA. (1) The chief complaint must be a progressive visuospatial or perceptual problem. (2) The subject must have a normal ophthalmologic examination within 3 months of presentation. (3) Visuospatial/perceptual deficits must be corroborated on neuropsychological testing of spatial/perceptual function. (4) Performance on testing of episodic memory (the Rey Auditory Verbal Learning Test was used for this study) [14] must be superior to (>1.0 Z score) performance on testing of visuospatial/perceptual function (the Rey-Osterrieth complex figure test was used) [15]. (5) The neuropsychological test battery must demonstrate that visuospatial/perceptual deficits are more severe than deficits in all other cognitive domains. Patients with symptoms suggestive of severe depression, an infarct or tumor in the occipital, parietal or temporal lobes on head MRI/CT that could have contributed to the presenting syndrome or with medical conditions that could interfere with cognitive performance were excluded.
Neurological assessments
All neurological assessments were performed by a behavioral neurologist (KAJ). Demographic variables collected included age, sex, education, handedness, race and disease duration. All patients underwent testing with the Mini-Mental State Examination (MMSE) [16], the Frontal Assessment Battery (FAB) [17], Frontal Behavior Inventory (FBI) [18], apraxia subset of the Western Aphasia Battery (WAB-apraxia) [19], 15-item Boston Naming test (BNT) [20], Movement Disorder Society-sponsored version of the Unified Parkinson’s Disease Rating Scale (parts I, II and III) (MDS-UPDRS) [21], Clinical Dementia Rating (CDR) [22], Neuropsychiatric Inventory (NPI) [23], and a test of famous faces’ recognition [24]. Calculation ability was assessed using the calculation subscore from the Montreal Cognitive Assessment Battery [25]. In addition, the presence/absence of visual hallucinations, rapid eye movement sleep behavior disorder (RBD) and poly-mini-myoclonus at the time of testing were recorded. Rapid eye movement sleep behavior disorder was considered present if the behavior met diagnostic criteria B for rapid eye movement sleep behavior disorder, defined as abnormal, wild flailing movements occurring during sleep (with sleep-related injuries) or movements that are potentially injurious or disruptive [26]. Two of the four patients with RBD had a polysomnography. One showed REM sleep without atonia consistent with RBD. The other had REM sleep with atonia but no non-supine REM sleep was captured. The presence of anomia was assessed using a cut-off of <12 on the BNT. The presence of simultanagnosia was assessed using the Ishihara color plates and the documentation of how many items were recognized on visual inspection of a picture with five overlapping items. Cutoff was below 6/6 for plates and below 5/5 on overlapping pictures based on performance of 10 normal controls that scored 100 % on both tests. Handwriting samples were assessed for evidence of dysgraphia (Fig. 1). The presence/absence of oculomotor apraxia and optic ataxia were assessed on neurological examination. Oculomotor apraxia was defined as the inability to voluntarily direct one’s gaze to a particular point. Optic ataxia was defined as the impairment of goal-directed hand movements towards visually presented targets. Poly-mini-myoclonus was defined as the presence of intermittent and irregular jerks that are visible predominantly in the fingers when the arm is held outstretched and the figures extended, with amplitudes of the jerks just sufficient to produce movements of the joints [27].

Examples of handwriting from three PCA patients. Note abnormally formed letters, abnormal spacing, and variations in letter size, consistent with apraxic dysgraphia
Image acquisition
All patients underwent PiB-PET scanning, while 17 (68 %) underwent FDG-PET, with both acquired using a PET/CT scanner (GE Healthcare, Milwaukee, Wisconsin) as previously described. PET images were acquired after injection of C-11 PiB (average = 596 MBq; range = 292–729 MBq, uptake period = 40 min) and F-18-FDG (average = 540 MBq; range = 366–399 MBq, uptake period = 30 min); both scans were performed as previously described on the same day with 1 h interval between acquisitions [24]. All patients also underwent a standardized MRI imaging protocol at 3.0 T, which included a 3D magnetization prepared rapid acquisition gradient echo (MPRAGE) sequence [24]. A global PiB standardized uptake value ratio (SUVR) was calculated for each PiB-PET scan as previously described [28], with a 1.5 cut-off used for beta-amyloid positivity.
PET analyses
The FDG-PET images were analyzed both at the individual and group-level. Individual maps of hypometabolism were generated using 3-dimensional stereotactic surface projections. The software package used to perform these analyses was CortexID (GE Healthcare, Waukesha, WI, USA). Automated average Z scores generated from Cortex ID were calculated for the following regions: lateral and medial frontal lobes, lateral and medial parietal lobes, temporal lobes, cingulate cortex, occipital lobe, and primary visual cortex. Hypometabolism was considered present if Z scores were greater than 2. Additionally, Z scores of 2–3 were considered moderate hypometabolism and >3 were considered severe hypometabolism.
Group-level analyses were performed using SPM5 [29]. The FDG-PET scan for each subject was co-registered to the subjects MPRAGE scan using 6 degrees-of-freedom registration. The automated anatomical labelling atlas [30] containing pons was propagated to native MPRAGE space. All voxels in the FDG-PET image were then divided by median uptake of the pons to form FDG uptake ratio images. The MPRAGE scans were then normalized to a customized template, and these normalization parameters were used to also transform the FDG-PET uptake ratio images onto the customized template. Voxel-level comparisons of FDG-PET were performed using two-sided t tests in SPM5. The group of PCA subjects was compared to an age and gender-matched group of 20 healthy controls that had undergone identical FDG-PET and MRI acquisitions. These comparisons were performed after correction for multiple comparisons using the false discovery rate (FDR) correction at p < 0.001.
Group-level analyses of the PiB-PET scans were also performed using SPM5. As above, the PiB-PET scans were co-registered to the subjects MPRAGE and transformed into customized template space using the normalization parameters from the MPRAGE normalization. All voxels in the PiB-PET images were divided by median uptake in the cerebellum before normalization. Two-sided t tests were used to compare the PCA subjects to the 20 healthy controls. These comparisons were performed after correction for multiple comparisons using the false discovery rate (FDR) correction at p < 0.001.
Early PCA
We subdivided the 25 PCA patients based on the median disease duration of the cohort (4 years) in order to assess clinical and FDG-PET features of those that had a short duration of ≤4 years (n = 13) and hence could be considered to have early PCA. Disease duration was defined as the time from the onset of the first symptom observed by the patient and the patient’s significant other (both had to agree) to the time of presentation. Ten early PCA patients had an FDG-PET scan performed ≤4 years after onset, available for analysis. Patterns of FDG-PET hypometabolism were compared between the group of early PCA patients and the 20 controls correcting for multiple comparisons using the FDR correction at p < 0.001 and between early PCA and the rest of the PCA cohort at p < 0.001 uncorrected.
Statistical analysis
We used JMP software version 10.0.0 (SAS Institute Inc., Cary, NC, USA) to perform statistical analyses. According to convention, statistical significance is represented at two-tailed alpha level of 0.05. Group differences for categorical variables were assessed with the χ 2 test and Fisher’s exact test as appropriate, while differences in continuous variables were assessed using the Kruskal–Wallis test. Spearman Correlation analyses were performed between neuropsychological and clinical symptoms and hypometabolism Z scores.
Results
We identified 25 PCA patients who fulfilled our research criteria for PCA. Two patients were excluded because they presented with aphasia rather than visuoperceptual deficits. The demographic features of all 25 patients are shown in Table 1.
Clinical findings
The clinical features of the cohort are shown in Table 2. The most common clinical features in the cohort were simultanagnosia, dysgraphia (Fig. 1), poly-mini-myoclonus and oculomotor apraxia. On neurological testing all scores fell within the normal- mildly affected range except for Ishihara plates in which the average score fell within the severely affected range.
Single subject FDG-PET analysis
The Z scores for hypometabolism and the number of affected patients are shown in Table 3. Severe hypometabolism was seen in the right parietal lobe in 16 (94.1 %) patients, left parietal lobe in 14 (82.4 %) extending through the right and left medial parietal lobes in 16 (94.1 %) and 14 (82.4 %) patients and finally involving the right and left occipital lobes in 14 (82.4 %) and 15 (88.2 %) patients. Mild hypometabolism was present in bilateral frontal and temporal lobes, extending through the left and right posterior cingulum, and the bilateral visual cortex. Both medial frontal cortices and anterior cingulum remained unaffected in all the patients of our cohort.
Group analysis of FDG-PET using SPM
The regions of hypometabolism observed in all 17 patients are shown in Fig. 2. There was reduced metabolism bilaterally throughout lateral parietal and occipital cortices, precuneus and posterior cingulate, lateral posterior temporal cortex and medial occipital cortex, particularly in the right hemisphere, compared to controls.

Three-dimensional brain renderings showing FDG-PET hypometabolism in the entire PCA cohort compared to controls (a), the early PCA subjects compared to controls (b), and early PCA compared to the rest of the PCA patients (c). Renders were generated using the BrainNet Viewer (http://www.nitrc.org/projects/bnv/)
Associations between classic PCA clinical features and FDG-PET
Simultanagnosia was associated with hypometabolism in the right occipital lobe (p = 0.0054), right posterior cingulum (p = 0.0186) and the right visual cortex (p = 0.0193). In contrast, optic ataxia was associated with hypometabolism in left occipital lobe (p = 0.0109) and left visual cortex (p = 0.0339) and oculomotor apraxia with left parietal lobe (p = 0.0357), left posterior cingulate gyrus (p = 0.0157) and left medial parietal cortex (p = 0.0175). There was no association between dysgraphia and acalculia and the hypometabolism patterns.
Early PCA
Demographic features were similar between early PCA and all PCA patients (Table 1). Only four features were present in more than 50 % of the early PCA patients including simultanagnosia, dysgraphia, poly-mini-myoclonus and oculomotor apraxia (Table 2). Only simultanagnosia was present in 85 % of the early PCA patients. The only feature than differed by more than 20 % between early PCA and the entire cohort was optic ataxia. Three patients had disease duration of less than 2 years of which two had simultanagnosia and poly-mini-myoclonus. Performance on neurological testing in early PCA was similar to performance in the entire PCA cohort although the early PCA patients were in general less cognitively impaired.
In the SPM analysis (Fig. 2), the early PCA group showed a similar pattern of hypometabolism to the entire cohort although there was less involvement of the occipital cortex in early PCA compared to the rest of the cohort.
PiB-PET analysis
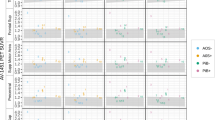
All 25 PCA patients had an SUVR ratio >1.50 and hence were amyloid positive. The average SUVR ratio for all 25 PCA patients was >2.19 (±0.35). Twenty of the 25 (90 %) PCA patients had an SUVR >2.00. The regional pattern of PiB-PET uptake is shown in Fig. 3. Widespread PiB-PET uptake was observed with most severe uptake in lateral and medial prefrontal, lateral temporal and medial parietal cortex.

Three-dimensional brain renderings showing PiB-PET uptake in the entire PCA cohort compared to controls. Renders were generated using the BrainNet Viewer (http://www.nitrc.org/projects/bnv/)
The average SUVR ratio of the early PCA patients was 2.08 (±0.31). Eleven of the 13 (87 %) early PCA patients had an SUVR ratio >2.00. There was no difference in SUVR ratio between early PCA and the rest of the PCA cohort.
Discussion
This is one of the largest prospective studies to date of a cohort of patients with a clinical diagnosis of PCA that underwent FDG-PET and amyloid PET imaging. The study identifies important clinical, cognitive and neuroimaging features of PCA.
While the clinical features of our PCA patients are unsurprisingly similar to previously reported PCA cohorts [2, 4, 13, 31–33], our study design allowed us to further refine the clinical syndrome of PCA. Our PCA cohort had an average age of onset of 60 years which might suggest that PCA should be considered an early onset dementia. However, we did not have any subjects presenting less than 45 years and hence PCA would not be considered a young onset dementia, based on our previous definitions [34]. Simultanagnosia was noted to be the most common clinical feature in our cohort in general, and was also the most common feature of early PCA, affecting 85 % of patients with disease duration of 4 years or less. Dysgraphia and oculomotor apraxia were also common features of PCA, and of early PCA. Poly-mini-myoclonus however, is not a feature that is considered, or typically assessed, in patients with PCA yet it was more common than some of the features typically associated with PCA, such as oculomotor apraxia and optic ataxia. We previously reported an association between poly-mini-myoclonus and PCA [35], although our previous study was retrospective in nature and clearly underestimated the frequency of this clinical feature compared to the current prospectively recruited cohort, which shows that poly-mini-myoclonus is a common feature of PCA. In contrast to simultanagnosia, oculomotor apraxia and poly-mini-myoclonus, our data suggested that optic ataxia, while relatively common in PCA, is a later feature of PCA. In fact, optic ataxia was not identified in early PCA. Anomia was also observed in our PCA cohort, as previously reported [4, 33, 35, 36], and is most likely due to involvement of the left temporal lobe. We also found that approximately 20 % of our cohort had visual hallucinations or RBD, with the frequency similar in early PCA and across the entire cohort. This suggests that hallucinations and RBD when associated with PCA are both likely to be observed early in the disease course. These two features are not frequently reported in PCA, but are suggestive of underlying Lewy body disease [7, 35], given these are classic features of dementia with Lewy bodies [37]. Acalculia, a feature of the Gerstmann’s syndrome, was striking and was also observed in early PCA. Prosopagnosia was noted to be present in some of the patients but was relatively mild when present in most instances and was most likely perceptual, as opposed to agnostic in nature. Neuropsychiatric, behavioral, executive and extrapyramidal features were noted to be absent to mild in PCA. Ideomotor apraxia was not a common feature and when present also appeared to be mild in most patients.
On FDG-PET analysis, we observed marked hypometabolism of the bilateral parietal and occipital lobes, showing involvement of these regions in more than 80 % of the PCA patients. Mild hypometabolism in bilateral frontal lobes, posterior cingulate and the bilateral visual cortex was observed in 50 % of the PCA patients. The bilateral anterior cingulate and medial frontal cortex appears to remain unaffected. These findings concur with previous PET studies [9–12]. All 25 PCA patients were amyloid positive with very high SUVR ratios. This suggest, with high certainty that the underlying pathology in all of our PCA patients is Alzheimer’s disease. It is also possible however, although less likely, that in some of our cases amyloid deposition is co-occurring with another pathology, such as corticobasal degeneration that has been reported in a couple of PCA patients [6]. It is also unlikely that our patients suffered from Creutzfeldt-Jakob disease, given the disease durations and the fact that amyloid imaging is negative in Creutzfeldt-Jakob disease [38]. Furthermore, large amplitude myoclonic jerks, a feature of Creutzfeldt-Jakob disease, was not observed in our cohort. Our PCA patients instead showed poly-mini-myoclonus. Therefore, our cohort is likely very homogeneous, pathologically, although it is possible that in some patients there is co-existing Lewy body pathology.
Our association analyses allowed us to investigate the hypometabolic associations of the clinical features observed in PCA. Simultanagnosia was associated with hypometabolism in the right occipital lobe, posterior cingulum and visual cortex. These findings are expected as simultanagnosia generally reflects the severity of damage in the visual associative cortex without the involvement of the lateral parietal cortex [2, 39]. However, in our study it was found to be associated only with right-sided involvement. Optic ataxia was associated with involvement of the left occipital and visual cortex, while oculomotor apraxia with left parietal lobe and posterior cingulum. These results further quantify the neural correlations of oculomotor apraxia to the posterior parietal cortices. In fact, an fMRI study recently reported finding an association between the lateral occipitoparietal junction (dorsal stream) and changes in graspable stimuli and visually guided reaching to grasp [40, 41]. The optic ataxia findings suggest that occipital lobe involvement needs to be present before this PCA feature will emerge. We did not find any association between two of the features of Gerstmann’s syndrome (acalculia and agraphia) with any hypometabolic patterns, which could be due a small sample size of our cohort; however, these findings have been shown to be associated with the left parietal cortex by another group [42].
One of the important aspects of our study was the assessment of clinical and FDG-PET features of early PCA. We observed little difference in early PCA compared to the entire cohort suggesting most features of PCA will be present early in the disease course. The only exception appeared to be optic ataxia which was not a feature of early PCA. Interestingly, the presence of optic ataxia was associated with left occipital lobe involvement which was a region found to be less affected in early PCA. And although we do not have longitudinal data, we can speculate that progressive involvement likely spreads from the right parietal lobe across to the left occipital lobe, which would explain the later emergence of optic ataxia.
All 25 PCA patients had SUVR ratios consistent with beta-amyloid deposition. Beta-amyloid is one of the two major proteins required for a pathological diagnosis of Alzheimer’s disease; tau being the other. Our group analysis of PiB did not show a regional pattern of beta-amyloid deposition unique to PCA. Prefrontal, temporal and medial parietal involvement has also been observed with other Alzheimer’s disease related syndromes [28, 43, 44]. The lack of beta-amyloid deposition being more striking in the occipitoparietal regions, mirroring the pattern of hypometabolism on FDG-PET, is consistent with pathological studies demonstrating greater tau, but not beta-amyloid deposition in these regions [4]. The subjects in this study all met clinical criteria for PCA [4, 13]. All subjects also met stringent research criteria for PCA. Given that we did not have any amyloid negative subjects in our cohort, it appears that our research criteria may be more specific to underlying Alzheimer’s disease than the clinical criteria, since other PCA cohorts have found subjects with non-Alzheimer’s pathologies [5, 6]. We have previously reported two subjects who presented with aphasia but were agnostic to their visual deficits [45]. Visuospatial/perceptual deficits were strikingly abnormal on neuropsychological testings and was the most severely impairment cognitive domain in both. Such subjects remain controversial in terms of classification. In fact, both were excluded from this study as they did not meet our research criteria for PCA.
The major strength of this study is the large number of PCA cases that were prospectively recruited and underwent amyloid and FDG-PET imaging. Another strength was the assessment of PCA subjects with short disease duration allowing the assessment of early features of PCA. A limitation of the study was that not all subjects underwent FDG-PET. In addition, pathological confirmation of Alzheimer’s disease was not available. The lack of autopsy also meant we could not confirm an association between the presence of hallucinations and RBD and co-existence of Lewy body disease.
References
Benson DF, Davis RJ, Snyder BD (1988) Posterior cortical atrophy. Arch Neurol 45(7):789–793
Kas A, de Souza LC, Samri D, Bartolomeo P, Lacomblez L, Kalafat M, Migliaccio R, Thiebaut de Schotten M, Cohen L, Dubois B, Habert MO, Sarazin M (2011) Neural correlates of cognitive impairment in posterior cortical atrophy. Brain 134(Pt 5):1464–1478
Beh SC, Muthusamy B, Calabresi P, Hart J, Zee D, Patel V, Frohman E (2014) Hiding in plain sight: a closer look at posterior cortical atrophy. Pract Neurol 15(1):5–13
Tang-Wai DF, Graff-Radford NR, Boeve BF, Dickson DW, Parisi JE, Crook R, Caselli RJ, Knopman DS, Petersen RC (2004) Clinical, genetic, and neuropathologic characteristics of posterior cortical atrophy. Neurology 63(7):1168–1174
Renner JA, Burns JM, Hou CE, McKeel DW Jr, Storandt M, Morris JC (2004) Progressive posterior cortical dysfunction: a clinicopathologic series. Neurology 63(7):1175–1180
Tang-Wai DF, Josephs KA, Boeve BF, Dickson DW, Parisi JE, Petersen RC (2003) Pathologically confirmed corticobasal degeneration presenting with visuospatial dysfunction. Neurology 61(8):1134–1135
Tang-Wai DF, Josephs KA, Boeve BF, Petersen RC, Parisi JE, Dickson DW (2003) Coexistent Lewy body disease in a case of “visual variant of Alzheimer’s disease”. J Neurol Neurosurg Psychiatry 74(3):389
Caroppo P, Belin C, Grabli D, Maillet D, De Septenville A, Migliaccio R, Clot F, Lamari F, Camuzat A, Brice A, Dubois B, Le Ber I (2015) Posterior Cortical Atrophy as an Extreme Phenotype of GRN Mutations. JAMA Neurol 72(2):224–228
Bokde AL, Pietrini P, Ibanez V, Furey ML, Alexander GE, Graff-Radford NR, Rapoport SI, Schapiro MB, Horwitz B (2001) The effect of brain atrophy on cerebral hypometabolism in the visual variant of Alzheimer disease. Arch Neurol 58(3):480–486
Nestor PJ, Caine D, Fryer TD, Clarke J, Hodges JR (2003) The topography of metabolic deficits in posterior cortical atrophy (the visual variant of Alzheimer’s disease) with FDG-PET. J Neurol Neurosurg Psychiatry 74(11):1521–1529
Schmidtke K, Hull M, Talazko J (2005) Posterior cortical atrophy: variant of Alzheimer’s disease? A case series with PET findings. J Neurol 252(1):27–35
Spehl TS, Hellwig S, Amtage F, Weiller C, Bormann T, Weber WA, Hull M, Meyer PT, Frings L (2014) Syndrome-specific patterns of regional cerebral glucose metabolism in posterior cortical atrophy in comparison to dementia with Lewy bodies and Alzheimer’s disease-A [F-18]-Fdg pet STUDY. J Neuroimaging 25(2):281–288
McMonagle P, Deering F, Berliner Y, Kertesz A (2006) The cognitive profile of posterior cortical atrophy. Neurology 66(3):331–338
Rey A (1958) L’examen clinique en psychologie./The clinical examination in psychology. Presses Universitaries De France, Oxford
Osterrieth PA (1944) Le test de copie d’une figure complexe:contribution a l’e´tude de la perception et de la memoire [The test of copying a complex figure: a contribution to the study of perception and memory]. Archive de Psychologie 30:286–350
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12(3):189–198
Dubois B, Slachevsky A, Litvan I, Pillon B (2000) The FAB: a frontal assessment battery at bedside. Neurology 55(11):1621–1626
Kertesz A, Davidson W, Fox H (1997) Frontal behavioral inventory: diagnostic criteria for frontal lobe dementia. Can J Neurol Sci 24(1):29–36
Kertesz A, Hooper P (1982) Praxis and language: the extent and variety of apraxia in aphasia. Neuropsychologia 20(3):275–286
Lansing AE, Ivnik RJ, Cullum CM, Randolph C (1999) An empirically derived short form of the Boston naming test. Arch Clin Neuropsychol 14(6):481–487
Goetz CG, Fahn S, Martinez-Martin P, Poewe W, Sampaio C, Stebbins GT, Stern MB, Tilley BC, Dodel R, Dubois B, Holloway R, Jankovic J, Kulisevsky J, Lang AE, Lees A, Leurgans S, LeWitt PA, Nyenhuis D, Olanow CW, Rascol O, Schrag A, Teresi JA, Van Hilten JJ, LaPelle N (2007) Movement disorder society-sponsored revision of the unified Parkinson’s disease rating scale (MDS-UPDRS): process, format, and clinimetric testing plan. Mov Disord 22(1):41–47
Morris JC (1993) The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology 43(11):2412–2414
Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J (1994) The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology 44(12):2308–2314
Josephs KA, Duffy JR, Strand EA, Machulda MM, Senjem ML, Master AV, Lowe VJ, Jack CR Jr, Whitwell JL (2012) Characterizing a neurodegenerative syndrome: primary progressive apraxia of speech. Brain 135(Pt 5):1522–1536
Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, Chertkow H (2005) The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 53(4):695–699
Sateia M (2005) The international classification of sleep disorders, 2nd edn. American Academy of Sleep Medicine, Weschester, NY
Wilkins DE, Hallett M, Erba G (1985) Primary generalised epileptic myoclonus: a frequent manifestation of minipolymyoclonus of central origin. J Neurol Neurosurg Psychiatry 48(6):506–516
Jack CR Jr, Lowe VJ, Senjem ML, Weigand SD, Kemp BJ, Shiung MM, Knopman DS, Boeve BF, Klunk WE, Mathis CA, Petersen RC (2008) 11C PiB and structural MRI provide complementary information in imaging of Alzheimer’s disease and amnestic mild cognitive impairment. Brain 131(Pt 3):665–680
Ashburner J, Friston KJ (2000) Voxel-based morphometry–the methods. Neuroimage 11(6 Pt 1):805–821
Tzourio-Mazoyer N, Landeau B, Papathanassiou D, Crivello F, Etard O, Delcroix N, Mazoyer B, Joliot M (2002) Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 15(1):273–289
Lehmann M, Crutch SJ, Ridgway GR, Ridha BH, Barnes J, Warrington EK, Rossor MN, Fox NC (2011) Cortical thickness and voxel-based morphometry in posterior cortical atrophy and typical Alzheimer’s disease. Neurobiol Aging 32(8):1466–1476
Mendez MF, Ghajarania M, Perryman KM (2002) Posterior cortical atrophy: clinical characteristics and differences compared to Alzheimer’s disease. Dement Geriatr Cogn Disord 14(1):33–40
Whitwell JL, Jack CR Jr, Kantarci K, Weigand SD, Boeve BF, Knopman DS, Drubach DA, Tang-Wai DF, Petersen RC, Josephs KA (2007) Imaging correlates of posterior cortical atrophy. Neurobiol Aging 28(7):1051–1061
Kelley BJ, Boeve BF, Josephs KA (2008) Young-onset dementia: demographic and etiologic characteristics of 235 patients. Arch Neurol 65(11):1502–1508
Josephs KA, Whitwell JL, Boeve BF, Knopman DS, Tang-Wai DF, Drubach DA, Jack CR Jr, Petersen RC (2006) Visual hallucinations in posterior cortical atrophy. Arch Neurol 63(10):1427–1432
Crutch SJ, Lehmann M, Warren JD, Rohrer JD (2013) The language profile of posterior cortical atrophy. J Neurol Neurosurg Psychiatry 84(4):460–466
McKeith IG, Dickson DW, Lowe J, Emre M, O’Brien JT, Feldman H, Cummings J, Duda JE, Lippa C, Perry EK, Aarsland D, Arai H, Ballard CG, Boeve B, Burn DJ, Costa D, Del Ser T, Dubois B, Galasko D, Gauthier S, Goetz CG, Gomez-Tortosa E, Halliday G, Hansen LA, Hardy J, Iwatsubo T, Kalaria RN, Kaufer D, Kenny RA, Korczyn A, Kosaka K, Lee VM, Lees A, Litvan I, Londos E, Lopez OL, Minoshima S, Mizuno Y, Molina JA, Mukaetova-Ladinska EB, Pasquier F, Perry RH, Schulz JB, Trojanowski JQ, Yamada M (2005) Diagnosis and management of dementia with Lewy bodies: third report of the DLB Consortium. Neurology 65(12):1863–1872
Villemagne VL, McLean CA, Reardon K, Boyd A, Lewis V, Klug G, Jones G, Baxendale D, Masters CL, Rowe CC, Collins SJ (2009) 11C-PiB PET studies in typical sporadic Creutzfeldt-Jakob disease. J Neurol Neurosurg Psychiatry 80(9):998–1001
Himmelbach M, Erb M, Klockgether T, Moskau S, Karnath HO (2009) fMRI of global visual perception in simultanagnosia. Neuropsychologia 47(4):1173–1177
Hinkley LB, Krubitzer LA, Padberg J, Disbrow EA (2009) Visual-manual exploration and posterior parietal cortex in humans. J Neurophysiol 102(6):3433–3446
Rice NJ, Valyear KF, Goodale MA, Milner AD, Culham JC (2007) Orientation sensitivity to graspable objects: an fMRI adaptation study. Neuroimage 36(Suppl 2):T87–T93
Rusconi E, Pinel P, Dehaene S, Kleinschmidt A (2010) The enigma of Gerstmann’s syndrome revisited: a telling tale of the vicissitudes of neuropsychology. Brain 133(Pt 2):320–332
Josephs KA, Duffy JR, Strand EA, Machulda MM, Senjem ML, Lowe VJ, Jack CR Jr, Whitwell JL (2014) APOE epsilon4 influences beta-amyloid deposition in primary progressive aphasia and speech apraxia. Alzheimers Dement 10(6):630–636
Lehmann M, Ghosh PM, Madison C, Laforce R Jr, Corbetta-Rastelli C, Weiner MW, Greicius MD, Seeley WW, Gorno-Tempini ML, Rosen HJ, Miller BL, Jagust WJ, Rabinovici GD (2013) Diverging patterns of amyloid deposition and hypometabolism in clinical variants of probable Alzheimer’s disease. Brain 136(Pt 3):844–858
Wicklund MR, Duffy JR, Strand EA, Whitwell JL, Machulda MM, Josephs KA (2013) Aphasia with left occipitotemporal hypometabolism: a novel presentation of posterior cortical atrophy? J Clin Neurosci 20(9):1237–1240
Acknowledgments
This study was funded by the Alzheimer’s Association (NIRG-12-242215, PI Whitwell). The authors would like to acknowledge Drs. Petersen, Boeve and Knopman, Mayo Clinic, Rochester, MN, for patient referral and Dr. Jack, Mayo Clinic, Rochester, MN for usage of his laboratory for PiB PET analyses.
Conflicts of interest
T. Singh and D. Drubach report no disclosures. K. Josephs is funded by NIH R01-DC010367 (PI), R01-AG037491 (PI), R01-DC012519 (Co-I), and the Alzheimer’s Association (Co-I). M. Machulda is funded by R01-AG037491 (Co-I), R01-DC012519 (Co-I), and the Alzheimer’s Association (Co-I). L. Apostolova serves on the Speakers Bureau for Lilly Pharmaceuticals and receives research funding from the NIH and the Easton Consortium for Alzheimer’s Drug Development and Biomarker Discovery. V. Lowe is a consultant for Bayer Schering Pharma and receives research support from GE Healthcare, Siemens Molecular Imaging, AVID Radiopharmaceuticals, the NIH, the Elsie and Marvin Dekelboum Family Foundation, the MN Partnership for Biotechnology and Medical Genomics, and the Leukemia & Lymphoma Society. J. Whitwell is funded by R01-DC012519 (PI), R01-DC010367 (Co-I), R01-AG037491 (Co-I), and the Alzheimer’s Association (PI).
Ethical standard
The study was approved by the Mayo Clinic institutional review board and all patients signed a consent form allowing their participation in the study. The research has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Singh, T.D., Josephs, K.A., Machulda, M.M. et al. Clinical, FDG and amyloid PET imaging in posterior cortical atrophy. J Neurol 262, 1483–1492 (2015). https://doi.org/10.1007/s00415-015-7732-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-015-7732-5