
Abstract
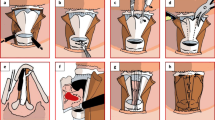
Ideal speech restoration remains a difficult challenge for patients undergoing laryngectomy so far. Our aim was to explore the feasibility of neoglottic reconstruction with sternohyoid muscles on upper-tracheal orifice after total laryngectomy which can obtain relatively ideal voice rehabilitation. Fifteen male patients are laryngectomized, of whom eight with standard total laryngectomy and seven underwent nonstandard total laryngectomy with epiglottis conserved. After laryngectomy, the upper margin of the anterior hypopharyngeal mucosa (postcricoid mucosa) was stitched to the posterior margin of upper-tracheal orifice and a triangle-shaped neoglottis on upper-tracheal orifice was reconstructed using bilateral sternohyoid muscles near the hyoid bone which were sutured to the posterior wall and bilateral of upper-tracheal orifice. Then tracheolingual root anastomosis was done and reconstruction surgery was completed. Finally, a satisfactory voice was achieved in 14 of 15 patients except one whose neoglottis is stenosed and 11 cases had no severe complications including aspiration erroneous deglutition. The stomach catheters were removed successfully from 4 to 6 weeks after surgery in 11 cases, respectively. The neoglottis had to be closed in three patients because of aspiration problem. One neoglottis was closed 3 weeks after surgical reconstruction because of tracheal rings tear which created a bigger neoglottis. One neoglottis was removed 32 moths after total laryngectomy due to big neoglottis. Another one was closed 3 weeks after surgery by reason of the fear of aspiration without psychological preparation. Therefore, it is feasible to use the sternohyoid muscles for creation of a neoglottis on upper-tracheal orifice and provide an alternative surgical method of the voice restoration for the patients after laryngectomy.


Similar content being viewed by others

References
Schwartz AW (1978) Dr. Theodor Billroth and the first laryngectomy. Ann Plast Surg 1(5):513–516
Sloane PM, Griffin JM, O’Dwyer TP (1991) Esophageal insufflation and video fluoroscopy for evaluation of esophageal speech in laryngectomy patients: clinical implications. Radiology 181(2):433–437
Aguiar-Ricz L, Dantas RO, Ricz H, Gielow I, Mamede RC, Perdoná GC (2007) Behavior of the cricopharyngeal segment during esophageal phonation in laryngectomized patients. J Voice 21(2):248–256
Clark JG, Stemple JC (1982) Assessment of three modes of alaryngeal speech with a synthetic sentence identification (SSI) task in varying message-to-competition ratios. J Speech Hear Res 25(3):333–338
Singer MI, Blom ED (1980) An endoscopic technique for restoration of voice after laryngectomy. Ann Otol Rhinol Laryngol 89(Pt 1):529–533
Arslan M (1972) Reconstructive laryngectomy. Report on the first 35 cases. Ann Otol Rhinol Laryngol 81(4):479–487
Vega MF (1975) Larynx reconstructive surgery—a study of three-year findings—a modified surgical technique. Laryngoscope 85(5):866–881
De Bodt MS, Van de Heyning PH, Wuyts FL, Lambrechts L (1996) The perceptual evaluation of voice disorders. Acta Otorhinolaryngol Belg 50(4):283–291
Yamaguchi H, Shrivastav R, Andrews ML, Niimi S (2003) A comparison of voice quality ratings made by Japanese and American listeners using the GRBAS scale. Folia Phoniatr Logop 55(3):147–157
Elmiyeh B, Dwivedi RC, Jallali N, Chisholm EJ, Kazi R, Clarke PM, Rhys-Evans PH (2010) Surgical voice restoration after total laryngectomy: an overview. Indian J Cancer 47(3):239–247
Snidecor JC, Curry ET (1959) Temporal and pitch aspects of superior esophageal speech. Ann Otol Rhinol Laryngol 68:623–636
Salmon SJ (2005) Commonalities among alaryngeal speech methods. In: Doyl PC, Keith RL (eds) Contemporary considerations in the treatment and rehabilitation of head and neck cancer: voice, speech, and swallowing. Pro-ed, Austin, pp 59–74
Globlek D, Stajner-Katusic S, Musura M, Horga D, Liker M (2004) Comparison of alaryngeal voice and speech. Logoped Phoniatr Vocol 29(2):87–91
Maccallum JK, Cai L, Zhou L, Zhang Y, Jiang JJ (2009) Acoustic analysis of aperiodic voice: perturbation and nonlinear dynamic properties in esophageal phonation. J Voice 23(3):283–290
Geraghty JA, Wenig BL, Smith BE, Portugal LG (1996) Long-term follow-up of tracheoesophageal puncture results. Ann Otol Rhinol Laryngol 105(7):501–503
Ferrer Ramírez MJ, Guallart Doménech F, Brotons Durbán S, Carrasco Llatas M, Estellés Ferriol E, López Martínez R (2001) Surgical voice restoration after total laryngectomy: long-term results. Eur Arch Otorhinolaryngol 258(9):463–466
Laccourreye O, Ross J, Brasnu D, Chabardes E, Kelly JH, Laccourreye H (1994) Extended supracricoid partial laryngectomy with tracheocricohyoidoepiglottopexy. Acta Otolaryngol 114(6):669–674
Rizzotto G, Succo G, Lucioni M, Pazzaia T (2006) Subtotal laryngectomy with tracheohyoidopexy: a possible alternative to total laryngectomy. Laryngoscope 116(10):1907–1917
Pearson BW (1981) Subtotal laryngectomy. Laryngoscope 91(11):1904–1912
Acknowledgments
This project was funded by the Science and Technology Commission of Shanghai Municipality (Nos. 15401971600, 16411960600 and 16411950101).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The Ethical Committee of the Eye, Ear, Nose and Throat Hospital of Fudan University reviewed and approved the study protocol.
Conflict of interest
The authors have no conflict of interest to declare.
Additional information
CJ. Li and L. Cheng have the same contribution in this paper and they are co-first authors.
Rights and permissions
About this article

Cite this article
Li, C.J., Cheng, L., Wu, H. et al. Neoglottis reconstruction with sternohyoid muscles on upper-tracheal orifice after laryngectomy. Eur Arch Otorhinolaryngol 274, 383–388 (2017). https://doi.org/10.1007/s00405-016-4274-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-016-4274-0