
Abstract
Background
Little scientific evidence exists on blood loss and transfusion rates depending on the fixation technique. The hypothesis of this study was that the blood loss and transfusion rate are lower in cemented and hybrid total hip arthroplasty (THA) compared to cementless THA.
Methods
We retrospectively compared a total of 1500 patients who received either cementless, cemented, hybrid or reverse hybrid THA. All patients underwent THA in 2021 at a single orthopedic center in Germany.
Results
The lowest blood loss was found in patients who received a fully cemented THA (695 ± 74 ml). Hybrid THA with a cemented stem showed a blood loss of 845 ± 30 ml and reverse hybrid THA showed the highest blood loss with an average of 994 ± 74 ml. Cementless THA caused an average blood loss of 957 ± 16 ml. There was a significant difference between cementless THA, hybrid THA (cemented stem), and fully cemented THA (p < 0.05). Transfusion rates ranged from 1.3% (cementless THA) to 7.9% (cemented THA) between the groups with a transfusion rate of 2.5% overall.
Conclusion
We found significantly lower blood loss in cemented THA and hybrid THA compared to cementless THA. Although blood loss was lower in cemented and hybrid THA, this did not result in lower transfusion rates. This could be due to other confounders such as age, comorbidities, and preoperative anemia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Total hip arthroplasty (THA) is one of the most successful orthopedic surgeries of the past century with good to excellent long-term results [1]. In Germany in 2020, 95,9% of all THA performed were primary [2].
In other European countries, such as Sweden, cemented fixation is the most common fixation technique because of poor results of cementless fixation during the 1990s. However, in recent years with improved implants, cementless fixation was regaining popularity. In 2019, the cementless implantation technique was used in 27.8% of all THAs in Sweden [3].
In contrast to that, the majority of THA are implanted in a cementless press-fit technique in Germany. In 2020, the German Arthroplasty Registry (EPRD) showed that 77.6% of all THAs were implanted without cement [2]. Cemented fixation of the femoral component (Hybrid THA) is more common in elderly patients. In Germany, the mean age of patients who underwent cementless primary THA was 67 years in 2020. For hybrid THA, it was 79 years, and for cemented fixation, it was 81 years [2].
The estimated blood loss after THA is reported to be between 900 and 1500 ml [4, 5]. Studies report transfusion rates of up to 69% [6], but with new surgical approaches and the implementation of patient blood management protocols, this has been reduced to about 10% in recent years [7].
High blood loss could result in anemia and the need for allogeneic blood transfusions (ABT). ABT are also associated with risks, such as pathogen transmission, immunomodulation, or transfusion-related lung injury (TRALI) [8, 9]. In addition, anemia is associated with increased morbidity and even mortality [10, 11]. Blood-saving measures, such as the use of tranexamic acid, led to a reduction in blood loss [12,13,14,15]. Other possibilities should be assessed to further reduce blood loss. Therefore, patient blood management (PBM) gained more interest and improved patient outcomes [16]. PBM includes preoperative optimization of hemoglobin levels (Hb), standardized transfusion protocols, and blood-sparing techniques [16].
This study investigates whether blood loss depends on the THA fixation technique and, if so, whether blood loss is lower in hybrid or cemented THA compared to cementless THA. We hypothesized that blood loss is lower in cemented and hybrid THA than in cementless THA.
Materials and methods
Retrospectively 1500 consecutive patients who underwent primary THA in 2021 in a single German orthopedic center were reviewed. All patients were included in this study. One thousand one hundred and twenty-nine of these patients received cementless THA (group 1), thirty-eight patients cemented (group 2), and three hundred and thirty-three received hybrid (two hundred and ninety-four; group 3) or reverse hybrid THA (thirty-nine; group 4). For all patients, the same minimally invasive anterolateral approach was used. In all patients, the same PMMA cement was used if applicable (Palacos®, Heraeus Medical GmbH, Wehrheim, Germany). Cemented fixation was used in patients over 80 years of age, if clinically evident osteoporosis was present or if primary implant stability was not achieved using the press-fit technique. All patients were preoperatively evaluated in terms of anemia and in the case of iron deficiency substituted (1 g Ferinject® i.v., Vifor Pharma Deutschland GmbH, München, Germany). All patients were warmed pre-, peri- and post-operatively with an active heating system and warmed i.v. fluids according to the hospital standard.
Blood-saving measures included use of tranexamic acid if no contraindications were present (preoperative: orally 1 g or 1.5 g if > 100 kg body weight, 1 g topical and 500 mg 1–1–1 orally post-operatively for 2 days). No drains were used. If necessary, anti-plated therapy was continued, according to individual risk management. All patients received NSAID with selective COX-2 blockers as pain medication if no terminal kidney disease or other contraindications were present. No patients with terminal kidney disease were treated in our institution, due to a lack of dialysis resources. Low-molecular-weight heparin (LMWH, 40 mg once daily) was used as a thromboembolic prophylaxis according to the German guidelines. Preoperatively, hemoglobin concentration (Hb) and hematocrit values (Hk) were routinely obtained 1 day before surgery. Postoperatively, Hb and Hk were routinely obtained on the first and third post-operative days. Blood loss was calculated using the Hb balance method [17] and blood volume using Nadler’s formula [18]:
Blood volume was assumed using the formula of Nadler et al.
with k1 = 0,3669, k2 = 0,03,219, k3 = 0,6041 for men and k1 = 0,3561, k2 = 0,03,308, k3 = 0,1833 for women.
All blood transfusions were recorded. The indication for blood transfusion was Hb < 4.8 g/dl and cardiovascular symptoms with hypotension and tachycardia. All data for this study were obtained from the institutional database. Furthermore, complication statistics were reviewed in regard to major bleeding events such as gastrointestinal bleedings and ulceration.
Statistical methods
Statistical analysis was performed with SPSS® (Version 27). A nonrepeated ANOVA was used to compare blood loss between the groups. Furthermore, Bonferroni and two-sided paired Student's t tests were used to compare blood loss between the different groups. p values < 0.05 were considered significant. All values are presented as means with standard error of mean or mean with range (age, body mass index).
Results
The mean age of all patients was 68.7 years (20–93 years), mean body mass index (BMI) was 28.9 kg/m2 (17.7–50.6 kg/m2).
Group 1 was the largest group with 1129 patients who received cementless THA (75.2%). The smallest group was group 2 with only 38 patients (2.5%) with fully cemented THA. With 294 patients, the second largest group accounted for group 3 who received a hybrid THA, and 39 patients in group 4 received a reverse hybrid THA. The groups were significantly different in ASA, BMI, and age. Post hoc analysis with Bonferroni tests showed significant differences between group 1 compared to group 2 and 3. The patients in groups 2 and 3 were older (p < 0.001), weighed less (BMI, p < 0.001), and were sicker (ASA, p < 0.05) than the patients in group 1 (Table 1).
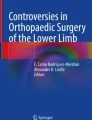
The calculated blood loss in group 1 (cementless THA) was 957 ± 16 ml. Blood loss in group 2 (cemented THA) was lowest at 695 ± 74 ml and in group 3 (hybrid THA) 845 ± 30 ml. Group 4 had the highest calculated blood loss with 994 ± 74 ml (Table 2, Fig. 1).

Calculated blood loss in comparison between cementless, cemented, hybrid, and reverse hybrid THA
The ANOVA analysis showed significant differences in the calculated blood loss between the groups (p < 0.005). Post hoc analysis with Bonferroni testing showed that blood loss between reverse hybrids was not significantly different from blood loss in cementless THA (p = 1.0). Group 2 (p = 0.012) and group 3 (p = 0.021) had significantly lower blood loss compared to group 1. The difference in calculated blood loss between groups 2 and 3 was not significant (p = 0.087) (Table 3). A total of 37 of the 1500 patients received a blood transfusion (2.5%). Of these, 15 received a cementless THA (transfusion rate 1.3%). Nineteen patients with partially cemented THA received a transfusion, seventeen with hybrid THA (transfusion rate 5.8%), and two with reverse hybrid THA (transfusion rate 5.1%). The highest transfusion rate was found in patients who received cemented THA (3/39 patients, transfusion rate 7.9%). No major bleeding events occurred during the study period.
Discussion
This study investigated the calculated blood loss and transfusion rates in THA using different fixation techniques. Blood loss was significantly lower in cemented THA and hybrid THA compared to cementless THA (p < 0.05). The overall transfusion rate was 2.5%.
Many studies have reported in the past that THA leads to substantial blood loss [18, 19]. This often requires ABT [6, 18, 19]. The demographic change in western societies leads to a growing number of elderly patients [20]. Consequently, until the COVID-19 pandemic, the numbers of THA performed per year were constantly increasing [2, 20] and projections show an increase of 27% from 2010 to 2040 [20]. Hence, a higher absolute demand for allogeneic blood is expected.
As blood transfusion is common in THA, individual health risks associated with ABT should be considered. In general, ABT is associated with increased morbidity, mortality, and costs [10, 11]. To improve the patient's outcome and lower complication rates, PBM is a key factor in elective THA. Minimizing blood loss and thus minimizing transfusion is crucial in THA.
The transfusion rate in this study was 2.5% on average, ranging from 1.3% to 7.9%. Higher transfusion rates in patients receiving a hybrid or fully cemented THA, while losing less blood might be explainable due to preoperative lower Hb values (Table 2). Studies have shown in the past that preoperative low Hb values can result in higher transfusion rates [21]. Compared to previous reports with transfusion rates of up to 69% [6, 18, 19], the transfusion rate in this study was low. Hochreiter et al. described transfusion rates between 8% and 15.8% comparing 124 patients in 2 groups using an anterolateral approach with cementless short-stem or straight-stem design with calculated blood loss between 1139 and 1358 ml, respectively [18]. Compared to our findings, the calculated blood loss was higher. Due to the different sample sizes and the different equations used to determine the actual blood loss, assessing blood loss and comparability between studies is difficult [22]. Wong et al. found transfusion rates of 23% in their prospective observational study of 787 patients [23]. Demey et al. evaluated the influence of femoral cementing in their study of 130 patients who underwent total knee arthroplasty (TKA) and found no difference between the groups [24]. To our knowledge, there are no comparative studies evaluating the influence of cementing in THA.
A considerable limitation of this study is the retrospective design and differences in group sizes. Although the total number of patients included in this study is quite large, the group size ranges from 38 to 1129 patients. Additionally, an individual indication for blood transfusion cannot be ruled out. Although there is a threshold for transfusion with an Hb level of 4.8 g/dl and lower, clinical symptoms could influence the decision to transfusion in patients with higher Hb levels.
Furthermore, not all factors could be assessed in this study. With regard to possible other confounding medication, such as anti-plated therapy or usage of NSAID, the literature reports no effect of such medication on blood loss in primary arthroplasty [25,26,27]. Chronic kidney disease (CDK) was not assessed in this study as a possible confounder. Though, recent studies showed no negative effects on transfusion rates in an adjusted PBM protocol for patients [28]. There were no major bleeding events found in our complication records for the study period, so a possible influence on transfusion rate can be ruled out.
Conclusion
Although other confounders might influence transfusion rates and blood loss, such as BMI, comorbidities, preoperative Hb levels, use of tranexamic acid and approach, this study shows the effect of PMMA bone cement for femoral fixation on blood loss in THA. Therefore, femoral stem cementing should be considered in the elderly patient with comorbidities to minimize blood loss.
Data availability
The datasets generated during and/or analyzed during the current study are available from corresponding author on reasonable request.
References
Lombardi AV Jr, Berend KR, Mallory TH, Skeels MD, Adams JB (2009) Survivorship of 2000 tapered titanium porous plasma-sprayed femoral components. Clin Orthop Relat Res 467(1):146–154
Alexander Grimberg VJ, Jörg Lützner OM, Michael M, Arnd S (2022) EPRD Jahresbericht 2021. https://doi.org/10.36186/reporteprd042021
Kärrholm JR, Cecilia; Naucler, Emma, Nåtman J, Vinblad J, Mohaddes M, Rolfson O (2021) Swedish Hip Arthroplasty Register Annual report 2019. https://doi.org/10.18158/H1BdmrOWu
Carling MS, Jeppsson A, Eriksson BI, Brisby H (2015) Transfusions and blood loss in total hip and knee arthroplasty: a prospective observational study. J Orthop Surg Res 10:48
Wei W, Wei B (2014) Comparison of topical and intravenous tranexamic acid on blood loss and transfusion rates in total hip arthroplasty. J Arthroplasty 29(11):2113–2116
Rosencher N, Kerkkamp HEM, Macheras G, Munuera LM, Menichella G, Barton DM, Cremers S, Abraham IL, Investigation FTO (2003) Orthopedic surgery transfusion hemoglobin European overview (OSTHEO) study: blood management in elective knee and hip arthroplasty in Europe*. Transfusion 43(4):459–469
Komnos GA, Manrique J, Foltz C, Klement MR, Restrepo C, Parvizi J (2021) Transfusion rates in total hip arthroplasty are lower in patients with direct anterior approach. Arch Bone Jt Surg 9(6):659–664
Spiess BD (2004) Transfusion of blood products affects outcome in cardiac surgery. Semin Cardiothorac Vasc Anesth 8(4):267–281
Rawn J (2008) The silent risks of blood transfusion. Curr Opin Anaesthesiol 21(5):664–668
Koch CG, Li L, Sun Z, Hixson ED, Tang A, Phillips SC, Blackstone EH, Henderson JM (2013) Hospital-acquired anemia: prevalence, outcomes, and healthcare implications. J Hosp Med 8(9):506–512
Musallam KM, Tamim HM, Richards T, Spahn DR, Rosendaal FR, Habbal A, Khreiss M, Dahdaleh FS, Khavandi K, Sfeir PM et al (2011) Preoperative anaemia and postoperative outcomes in non-cardiac surgery: a retrospective cohort study. Lancet 378(9800):1396–1407
Magill P, Hill JC, Bryce L, Martin U, Dorman A, Hogg R, Campbell C, Gardner E, McFarland M, Bell J et al (2021) Oral tranexamic acid for an additional 24 hours postoperatively versus a single preoperative intravenous dose for reducing blood loss in total hip arthroplasty: results of a randomized controlled trial (TRAC-24). Bone Joint J 103(7):1197–1205
Lee QJ, Chang WY, Wong YC (2017) Blood-sparing efficacy of oral tranexamic acid in primary total hip arthroplasty. J Arthroplasty 32(1):139–142
Yue C, Kang P, Yang P, Xie J, Pei F (2014) Topical application of tranexamic acid in primary total hip arthroplasty: a randomized double-blind controlled trial. J Arthroplasty 29(12):2452–2456
Hsu CH, Lin PC, Kuo FC, Wang JW (2015) A regime of two intravenous injections of tranexamic acid reduces blood loss in minimally invasive total hip arthroplasty: a prospective randomised double-blind study. Bone Joint J 97(7):905–910
Meybohm P, Herrmann E, Steinbicker AU, Wittmann M, Gruenewald M, Fischer D, Baumgarten G, Renner J, Van Aken HK, Weber CF et al (2016) Patient blood management is associated with a substantial reduction of red blood cell utilization and safe for patient’s outcome: a prospective, multicenter cohort study with a noninferiority design. Ann Surg 264(2):203–211
Foss NB, Kehlet H (2006) Hidden blood loss after surgery for hip fracture. J Bone Joint Surg Br 88(8):1053–1059
Hochreiter J, Hejkrlik W, Emmanuel K, Hitzl W, Ortmaier R (2017) Blood loss and transfusion rate in short stem hip arthroplasty a comparative study. Int Orthopaed 41(7):1347–1353
Carling MS, Jeppsson A, Eriksson BI, Brisby H (2015) Transfusions and blood loss in total hip and knee arthroplasty: a prospective observational study. J Orthopaed Surg Res. https://doi.org/10.1186/s13018-015-0188-6
Pilz V, Hanstein T, Skripitz R (2018) Projections of primary hip arthroplasty in Germany until 2040. Acta Orthop 89(3):308–313
Loppini M, Cannata R, Pisano A, Morenghi E, Grappiolo G (2021) Incidence and predictors of blood transfusions in one-stage bilateral total hip arthroplasty: a single center prospective cohort study. Arch Orthop Trauma Surg 142(11):3549–3554
Gibon E, Courpied J-P, Hamadouche M (2013) Total joint replacement and blood loss: what is the best equation? Int Orthop 37(4):735–739
Wong S, Tang H, De Steiger R (2015) Blood management in total hip replacement: an analysis of factors associated with allogenic blood transfusion. ANZ J Surg 85(6):461–465
Demey G, Servien E, Pinaroli A, Lustig S, Si Selmi TA, Neyret P (2010) The influence of femoral cementing on perioperative blood loss in total knee arthroplasty: a prospective randomized study. JBJS 92(3):536–541
Winkler SH, Barta S, Kehl V, Schroter C, Wagner F, Grifka J, Springorum HR, Craiovan B (2016) Perioperative blood loss and gastrointestinal tolerability of etoricoxib and diclofenac in total hip arthroplasty (ETO-DIC study): a single-center, prospective double-blinded randomized controlled trial. Curr Med Res Opin 32(1):37–47
Schwab P-E, Lavand’Homme P, Yombi J, Thienpont E (2017) Aspirin mono-therapy continuation does not result in more bleeding after knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 25(8):2586–2593
Li Z, Xiang S, Du Y, Zhang M, Bian Y, Feng B, Weng X (2022) Preoperative use of aspirin in total knee arthroplasty: safe or not? Orthop Surg 14(8):1673–1680
Hourlier H, Fennema P (2021) Application of an adjusted patient blood management protocol in patients undergoing elective total hip arthroplasty: towards a zero-percent transfusion rate in renal patients—results from an observational cohort study. J Orthopaed Surg Res. https://doi.org/10.1186/s13018-021-02846-z
Funding
No funding was received for the present study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Prof. Andreas Halder and Dr. Daniel Schrednitzki declare royalties from ZimmerBiomet and Depuy. They declare paid presentations for ZimmerBiomet and Depuy. Mr. N. Meißner declares no conflict of interest related to the present study.
Ethical approval
No IRB approval was necessary for this study, as this study presents the collection, analysis, and publication of retrospectively obtained and anonymized data. No sensible data were presented in this study.
Informed consent
All patients signed an informed consent for the surgical procedure.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Meißner, N., Halder, A.M. & Schrednitzki, D. Cemented and hybrid total hip arthroplasty lead to lower blood loss in primary total hip arthroplasty: a retrospective study. Arch Orthop Trauma Surg 143, 6447–6451 (2023). https://doi.org/10.1007/s00402-023-04851-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-023-04851-9