
Abstract
Background
Posttraumatic osteoarthritis (PTOA) following a tibial plateau fracture (TPF) is a debilitating disease which often affects a young and active patient population for whom good knee function is essential. Frequently, total knee arthroplasty (TKA) is the only surgical option. The aim of this systematic review was to evaluate functional outcome for TKA in PTOA patients, together with several secondary outcome parameters.
Methods
A systematic review according to the PRISMA guidelines was conducted. Studies were included that reported on patient-reported outcome measures, range of motion or objective functional analysis after TKA because of PTOA following TPF.
Results
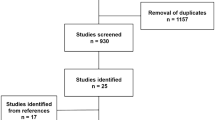
After analyzing 105 studies, 5 were included for the final review. In total, 162 patients with a TKA for PTOA were included of whom 125 (77%) were managed operatively for their TPF. All studies reported improvements in functional outcome after TKA, with two studies showing no significant differences between PTOA patients and a matched cohort of primary OA patients. Reported complication and re-intervention rates were higher for TKA patients with PTOA.
Conclusion
The results of this review indicate the TKA for PTOA after a TPF provides satisfactory functional outcome, with results similar to those of matched primary OA patients. TKA should, therefore, be considered a viable treatment option to improve function, but both patients and orthopedic surgeons should be aware of the higher complication rates in this patient population.

Similar content being viewed by others


References
Hap DXF, Kwek EBK (2020) Functional outcomes after surgical treatment of tibial plateau fractures. J Clin Orthop Trauma 11:S11–S15. https://doi.org/10.1016/j.jcot.2019.04.007
Civinini R, Carulli C, Matassi F et al (2009) Total knee arthroplasty after complex tibial plateau fractures. Chir Organi Mov 93:143–147. https://doi.org/10.1007/s12306-009-0033-3
Saleh KJ, Sherman P, Katkin P et al (2001) Total knee arthroplasty after open reduction and internal fixation of fractures of the tibial plateau. A minimum five-year follow-up study. J Bone Jt Surg - Ser A 83:1144–1148. https://doi.org/10.2106/00004623-200108000-00002
Softness KA, Murray RS, Evans BG (2017) Total knee arthroplasty and fractures of the tibial plateau. World J Orthop 8:107. https://doi.org/10.5312/wjo.v8.i2.107
Rowsell M, Gale D (2005) Total knee arthroplasty following internal fixation of a tibial plateau fracture. Inj Extra 36:352–354. https://doi.org/10.1016/j.injury.2004.12.065
Wasserstein D, Henry P, Paterson JM et al (2014) Risk of total knee arthroplasty after operatively treated tibial plateau fracture. J Bone Jt Surgery-American 96:144–150. https://doi.org/10.2106/JBJS.L.01691
Lizaur-Utrilla A, Collados-Maestre I, Miralles-Muñoz FA, Lopez-Prats FA (2015) Total knee arthroplasty for osteoarthritis secondary to fracture of the tibial plateau. a prospective matched cohort study. J Arthroplasty 30:1328–1332. https://doi.org/10.1016/j.arth.2015.02.032
Abdel MP, von Roth P, Cross WW et al (2015) Total knee arthroplasty in patients with a prior tibial plateau fracture: a long-term report at 15 years. J Arthroplasty 30:2170–2172. https://doi.org/10.1016/j.arth.2015.06.032
Scott CEH, Davidson E, Macdonald DJ et al (2015) Total knee arthroplasty following tibial plateau fracture a matched cohort study. Bone Jt J 97:550–557. https://doi.org/10.1302/0301-620X.97B4
Shamseer L, Moher D, Clarke M et al (2015) Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015: Elaboration and explanation. BMJ. https://doi.org/10.1136/bmj.g7647
Slim K, Nini E, Forestier D et al (2003) Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ J Surg 73:712–716. https://doi.org/10.1046/j.1445-2197.2003.02748.x
Marx RG, Wilson SM, Swiontkowski MF (2015) Updating the assignment of levels of evidence. J Bone Jt Surg 97:1–2. https://doi.org/10.2106/JBJS.N.01112
Noble PC, Scuderi GR, Brekke AC et al (2012) Development of a new knee society scoring system. Clin Ortho Relat Res. Springer, New York LLC, pp 20–32
Insall JN, Ranawat CS, Aglietti P, Shine J (1976) A comparison of four models of total knee-replacement prostheses. J Bone Joint Surg Am 58:754–765. https://doi.org/10.1097/00003086-199910000-00002
Dawson J, Fitzpatrick R, Murray D, Carr A (1998) Questionnaire on the perceptions of patients about total knee replacement. J Bone Jt Surg - Ser B 80:63–69. https://doi.org/10.1302/0301-620X.80B1.7859
Scuderi GR, Tria AJ (2002) Surgical techniques in total knee arthroplasty. Springer, New York
Weiss NG, Parvizi J, Trousdale RT et al (2003) Total knee arthroplasty in patients with a prior fracture of the tibial plateau. J Bone Jt Surg 85A:218–221. https://doi.org/10.1016/j.arth.2015.06.032
Aurich M, Koenig V, Hofmann G (2018) Comminuted intraarticular fractures of the tibial plateau lead to posttraumatic osteoarthritis of the knee: Current treatment review. Asian J Surg 41:99–105. https://doi.org/10.1016/j.asjsur.2016.11.011
Shearer DW, Chow V, Bozic KJ et al (2013) The predictors of outcome in total knee arthroplasty for post-traumatic arthritis. Knee 20:432–436. https://doi.org/10.1016/j.knee.2012.12.010
Wang X, Zhou Y, Shao H et al (2020) Total knee arthroplasty in patients with prior femoral and tibial fractures: outcomes and risk factors for surgical site complications and reoperations. Orthop Surg 12:210–217. https://doi.org/10.1111/os.12610
Fransen BL, Mathijssen NMC, Slot K et al (2019) Gait quality assessed by trunk accelerometry after total knee arthroplasty and its association with patient related outcome measures. Clin Biomech (Bristol, Avon) 70:192–196. https://doi.org/10.1016/j.clinbiomech.2019.10.007
Saleh H, Yu S, Vigdorchik J, Schwarzkopf R (2016) Total knee arthroplasty for treatment of post-traumatic arthritis: Systematic review. World J Orthop 7:584. https://doi.org/10.5312/wjo.v7.i9.584
Bourne RB, Chesworth BM, Davis AM et al (2010) Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res 468:57–63. https://doi.org/10.1007/s11999-009-1119-9
van Hove RP, Brohet RM, van Royen BJ, Nolte PA (2016) High correlation of the Oxford Knee Score with postoperative pain, but not with performance-based functioning. Knee Surg Sport Traumatol Arthrosc 24:3369–3375. https://doi.org/10.1007/s00167-015-3585-9
Moonot P, Medalla G, Matthews D et al (2009) Correlation between the oxford knee and american knee society scores at mid-term follow-up. J Knee Surg 22:226–230. https://doi.org/10.1055/s-0030-1247753
Liebensteiner MC, Herten A, Gstoettner M et al (2008) Correlation between objective gait parameters and subjective score measurements before and after total knee arthroplasty. Knee 15:461–466. https://doi.org/10.1016/j.knee.2008.07.001
Funding
No funding was received to assist with the preparation of this manuscript. The authors have no relevant financial or non-financial interests to disclose. The authors have no conflicts of interest to declare that are relevant to the content of this article. All the authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript. The authors have no financial or proprietary interests in any material discussed in this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose. The authors did not receive support from any organization for the submitted work. No funding was received to assist with the preparation of this manuscript. No funding was received for conducting this study. No funds, grants, or other support was received.
Ethical approval
This is a systematic review. No ethical approval is required.
Informed consent
This is a systematic review. Informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix A Search string
((((“Osteoarthritis, Knee”[Mesh] OR Knee Osteoarthritis* [tiab] OR Posttraumatic Osteoarthritis* [tiab] OR Osteoarthritis* [tiab] OR Traumatic Arthritis* [tiab]))) AND ((“Arthroplasty, Replacement, Knee”[Mesh] OR Knee Replacement Arthroplast* [tiab] OR Arthroplast* [tiab] OR Total Knee Arthroplast* [tiab] OR Total Knee Replacement* [tiab] OR Knee Arthroplast* [tiab] OR TKA* [tiab] OR Joint Replacement* [tiab]))) AND ((“Tibial Fractures”[Mesh] OR Tibial Fracture* [tiab] OR “Tibial Fracture” [Mesh] OR Tibial Plateau Fracture* [tiab])).
Appendix B Methodological items for non-randomized studies score (MINORS)
Author | Civinini | Lizaur | Saleh | Scott | Weiss | |
|---|---|---|---|---|---|---|
1 | A clearly stated aim The question addressed should be precise and relevant in the light of available literature | 1 | 2 | 1 | 2 | 2 |
2 | Inclusion of consecutive patients All patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion) | 2 | 2 | 2 | 2 | 2 |
3 | Prospective collection of data Data were collected according to a protocol established before the beginning of the study | 0 | 2 | 1 | 2 | 2 |
4 | Endpoints appropriate to the aim of the study Unambiguous explanation of the criteria used to evaluate the main outcome which should be in accordance with the question addressed by the study. In addition, the endpoints should be assessed on an intention-to-treat basis | 2 | 2 | 1 | 2 | 2 |
5 | Unbiased assessment of the study endpoint Blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated | 0 | 1 | 0 | 0 | 0 |
6 | Follow-up period appropriate to the aim of the study The follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events | 2 | 2 | 2 | 2 | 2 |
7 | Loss to follow-up less than 5% All patients should be included in the follow-up. Otherwise, the proportion lost to follow-up should not exceed the proportion experiencing the major endpoint | 1 | 2 | 2 | 2 | 1 |
8 | Prospective calculation of the study size Information of the size of detectable difference of interest with a calculation of 95% confidence interval, according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes | 0 | 1 | 0 | 1 | 0 |
Additional criteria in the case of comparative study | ||||||
9 | An adequate control group Having a gold-standard diagnostic test or therapeutic intervention recognized as the optimal intervention according to the available published data | n/a | 2 | n/a | 2 | n/a |
10 | Contemporary groups Control and studied group should be managed during the same time period (no historical comparison) | n/a | 2 | n/a | 1 | n/a |
11 | Baseline equivalence of groups The groups should be similar regarding the criteria other than the studied endpoints. Absence of confounding factors that could bias the interpretation of the results | n/a | 2 | n/a | 2 | n/a |
12 | Adequate statistical analyses Whether the statistics were in accordance with the type of study with calculation of confidence intervals or relative risk | n/a | 2 | n/a | 2 | n/a |
Total | 8/16 | 22/24 | 9/16 | 20/24 | 11/16 | |
Percentages | 50% | 92% | 56% | 83% | 69% | |
Rights and permissions
About this article

Cite this article
Pander, P., Fransen, B.L., Hagemans, F.J.A. et al. Functional outcome of total knee arthroplasty following tibial plateau fractures: a systematic review. Arch Orthop Trauma Surg 143, 1265–1274 (2023). https://doi.org/10.1007/s00402-021-04188-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-021-04188-1