
Abstract
Purpose
Regular follow-up for patients with Lynch syndrome (LS) is vital due to the increased risk of colorectal (50–80%), endometrial (40–60%), and other cancers. However, there is an ongoing debate concerning the best interval between colonoscopies. Currently, no specific endoscopic follow-up has been decided for LS patients who already have an index colorectal cancer (CRC). The aim of this study was to evaluate the risk of metachronous cancers (MC) after primary CRC in a LS population and to determinate if endoscopic surveillance should be more intensive.
Methods
A prospective cohort of patients with a confirmed diagnosis of hereditary CRC since 2009 was included. Patients with LS and a primary CRC were the cohort of choice.
Results
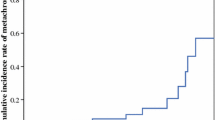
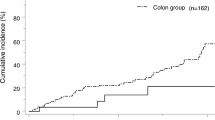
One hundred twenty-one patients were included with a median age of 44 years(16–70). At least one MC occurred in 39 patients (32.2%), with a median interval of 67 months (6–300) from index cancer. Fifteen (38.5%) developed two or more MCs during follow-up, with a median number of two (2–6) tumors occurring. Metachronous CRC were diagnosed after a median interval of 24 (6–57) months since last colonoscopy and were more commonly seen in MSH2 mutation carriers (58 vs. 35%, p = 0.001). After a median follow-up of 52.9 (3–72) months, no cancer-related deaths were recorded.
Conclusion
Patients with LS have an increased risk of MC, especially CRCs. With a median time period of 24 months between colonoscopy and metachronous CRC, the interval between surveillance colonoscopies following primary CRC should not exceed 18 months, especially in patients with MSH2 mutation.

Similar content being viewed by others

References
Stoffel EM (2010) Lynch syndrome/hereditary non-polyposis colorectal cancer (HNPCC). Minerva Gastroenterol Dietol 56:45–53
Moller P, Seppala T, Bernstein I, Holinski-Feder E, Sala P, Evans DG et al (2017) Cancer incidence and survival in Lynch syndrome patients receiving colonoscopic and gynaecological surveillance: first report from the prospective Lynch syndrome database. Gut 66:464–472
Lynch HT, Lynch PM, Lanspa SJ, Snyder CL, Lynch JF, Boland CR (2009) Review of the Lynch syndrome: history, molecular genetics, screening, differential diagnosis, and medicolegal ramifications. Clin Genet 76:1–18
Parry S, Win AK, Parry B, Macrae FA, Gurrin LC, Church JM, Baron JA, Giles GG, Leggett BA, Winship I, Lipton L, Young GP, Young JP, Lodge CJ, Southey MC, Newcomb PA, le Marchand L, Haile RW, Lindor NM, Gallinger S, Hopper JL, Jenkins MA (2011) Metachronous colorectal cancer risk for mismatch repair gene mutation carriers: the advantage of more extensive colon surgery. Gut 60:950–957
Schmeler KM, Lynch HT, Chen LM, Munsell MF, Soliman PT, Clark MB, Daniels MS, White KG, Boyd-Rogers SG, Conrad PG, Yang KY, Rubin MM, Sun CC, Slomovitz BM, Gershenson DM, Lu KH (2006) Prophylactic surgery to reduce the risk of gynecologic cancers in the Lynch syndrome. N Engl J Med 354:261–269
Vasen HF, Blanco I, Aktan-Collan K, Gopie JP, Alonso A, Aretz S et al (2013) Revised guidelines for the clinical management of Lynch syndrome (HNPCC): recommendations by a group of European experts. Gut 62:812–823
Giardiello FM, Allen JI, Axilbund JE, Boland CR, Burke CA, Burt RW et al (2014) Guidelines on genetic evaluation and management of Lynch syndrome: a consensus statement by the US Multi-Society Task Force on colorectal cancer. Gastroenterology 147:502–526
Auranen A, Joutsiniemi T (2011) A systematic review of gynecological cancer surveillance in women belonging to hereditary nonpolyposis colorectal cancer (Lynch syndrome) families. Acta Obstet Gynecol Scand 90:437–444
Jarvinen HJ, Mecklin JP, Sistonen P (1995) Screening reduces colorectal cancer rate in families with hereditary nonpolyposis colorectal cancer. Gastroenterology 108:1405–1411
Kalady MF, McGannon E, Vogel JD, Manilich E, Fazio VW, Church JM (2010) Risk of colorectal adenoma and carcinoma after colectomy for colorectal cancer in patients meeting Amsterdam criteria. Ann Surg 252:507–511 discussion 11-3
Canard G, Lefevre JH, Colas C, Coulet F, Svrcek M, Lascols O, Hamelin R, Shields C, Duval A, Fléjou JF, Soubrier F, Tiret E, Parc Y (2012) Screening for lynch syndrome in colorectal cancer: are we doing enough? Ann Surg Oncol 19:809–816
Heneghan HM, Martin ST, Winter DC (2015) Segmental vs extended colectomy in the management of hereditary nonpolyposis colorectal cancer: a systematic review and meta-analysis. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland 17:382–389
Karlitz JJ, Sherrill MR, DiGiacomo DV, Hsieh MC, Schmidt B, Wu XC et al (2016) Factors associated with the performance of extended colonic resection vs. segmental resection in early-onset colorectal cancer: a population-based study. Clin Transl Gastroenterol 7:e163
Haanstra JF, de Vos Tot Nederveen Cappel WH, Gopie JP, Vecht J, Vanhoutvin SA, Cats A, et al. Quality of life after surgery for colon cancer in patients with Lynch syndrome: partial versus subtotal colectomy. Dis Colon rectum 2012; 55: 653–659
Walters S, Maringe C, Butler J, Brierley JD, Rachet B, Coleman MP (2013) Comparability of stage data in cancer registries in six countries: lessons from the International Cancer Benchmarking Partnership. Int J Cancer 132:676–685
Fajobi O, Yiu CY, Sen-Gupta SB, Boulos PB (1998) Metachronous colorectal cancers. Br J Surg 85:897–901
Rajkumar T, Soumittra N, Pandey D, Nancy KN, Mahajan V, Majhi U (2004) Mutation analysis of hMSH2 and hMLH1 in colorectal cancer patients in India. Genet Test 8:157–162
Jarvinen HJ, Aarnio M, Mustonen H, Aktan-Collan K, Aaltonen LA, Peltomaki P et al (2000) Controlled 15-year trial on screening for colorectal cancer in families with hereditary nonpolyposis colorectal cancer. Gastroenterology 118:829–834
de Jong AE, Hendriks YM, Kleibeuker JH, de Boer SY, Cats A, Griffioen G et al (2006) Decrease in mortality in Lynch syndrome families because of surveillance. Gastroenterology 130:665–671
Mecklin JP, Aarnio M, Laara E, Kairaluoma MV, Pylvanainen K, Peltomaki P et al (2007) Development of colorectal tumors in colonoscopic surveillance in Lynch syndrome. Gastroenterology 133:1093–1098
Vasen HF, Abdirahman M, Brohet R, Langers AM, Kleibeuker JH, van Kouwen M et al (2010) One to 2-year surveillance intervals reduce risk of colorectal cancer in families with Lynch syndrome. Gastroenterology 138:2300–2306
Engel C, Rahner N, Schulmann K, Holinski-Feder E, Goecke TO, Schackert HK et al (2010) Efficacy of annual colonoscopic surveillance in individuals with hereditary nonpolyposis colorectal cancer. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association 8:174–182
Stuckless S, Green JS, Morgenstern M, Kennedy C, Green RC, Woods MO, Fitzgerald W, Cox J, Parfrey PS (2012) Impact of colonoscopic screening in male and female Lynch syndrome carriers with an MSH2 mutation. Clin Genet 82:439–445
Lecomte T, Cellier C, Meatchi T, Barbier JP, Cugnenc PH, Jian R et al (2005) Chromoendoscopic colonoscopy for detecting preneoplastic lesions in hereditary nonpolyposis colorectal cancer syndrome. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association 3:897–902
Hurlstone DP, Karajeh M, Cross SS, McAlindon ME, Brown S, Hunter MD et al (2005) The role of high-magnification-chromoscopic colonoscopy in hereditary nonpolyposis colorectal cancer screening: a prospective “back-to-back” endoscopic study. Am J Gastroenterol 100:2167–2173
Huneburg R, Lammert F, Rabe C, Rahner N, Kahl P, Buttner R et al (2009) Chromocolonoscopy detects more adenomas than white light colonoscopy or narrow band imaging colonoscopy in hereditary nonpolyposis colorectal cancer screening. Endoscopy 41:316–322
East JE, Suzuki N, Stavrinidis M, Guenther T, Thomas HJ, Saunders BP (2008) Narrow band imaging for colonoscopic surveillance in hereditary non-polyposis colorectal cancer. Gut 57:65–70
Stoffel EM, Turgeon DK, Stockwell DH, Zhao L, Normolle DP, Tuck MK, et al. Missed adenomas during colonoscopic surveillance in individuals with Lynch syndrome (hereditary nonpolyposis colorectal cancer). Cancer prevention research (Philadelphia), Pa) 2008; 1: 470–475
Niv Y, Moeslein G, Vasen HFA, Karner-Hanusch J, Lubinsky J, Gasche C et al (2014) Quality of colonoscopy in Lynch syndrome. Endoscopy International Open 2:E252–E2E5
Boland CR (2016) Recent discoveries in the molecular genetics of Lynch syndrome. Familial Cancer 15:395–403
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Anyla, M., Lefevre, J.H., Creavin, B. et al. Metachronous colorectal cancer risk in Lynch syndrome patients—should the endoscopic surveillance be more intensive?. Int J Colorectal Dis 33, 703–708 (2018). https://doi.org/10.1007/s00384-018-3004-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-018-3004-z