
Abstract
Purpose
Recently, Eggener et al. reignited a debate consisting to redefine Gleason Grade Group (GGG) 1 prostate cancer (PCa) as a precancerous lesion to reduce overdiagnosis and overtreatment. However, historical cohorts showed that some GGG1-labeled disease at biopsy may be underestimated by the standard PCa diagnostic workup. The aim was to assess whether the risk of adverse features at radical prostatectomy (RP) in selected GGG1 patients still exists in the era of pre-biopsy mpMRI and image-guided biopsies.
Methods
We retrospectively reviewed our data from a European RP dataset to assess in contemporary patients with GGG1 at mpMRI-targeted biopsy the rate of adverse features at final pathology, defined as ≥ pT3a and/or pN+ and/or GGG ≥ 3.
Results
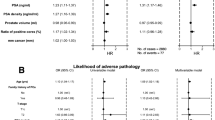
A total of 419 patients with cT1-T2 cN0 GGG1-PCa were included. At final pathology, 143 (34.1%) patients had adverse features. In multivariate analysis, only unfavorable intermediate-risk/high-risk disease (defined on PSA or stage) was predictive of adverse features (OR 2.45, 95% CI 1.11–5.39, p = 0.02). A significant difference was observed in the 3-year biochemical recurrence-free survival between patients with and without adverse features (93.4 vs 87.8%, p = 0.026). In sensitivity analysis restricted low- and favorable intermediate-risk PCa, 122/383 patients (31.8%) had adverse features and no preoperative factors were statistically associated with this risk.
Conclusion
In this European study, we showed that there is still a risk of underestimating GGG1 disease at biopsy despite the routine use of image-guided biopsies. Future studies are warranted to improve the detection of aggressive disease in GGG1-labeled patients by incorporating the latest tools such as genomic testing or radiomics.

Similar content being viewed by others


Availability of data and materials
Data are available upon request to the corresponding author.
Code availability
None.
References
Drost FH, Osses DF, Nieboer D et al (2019) Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst Rev 4(4):CD012663
Kasivisvanathan V, Rannikko AS, Borghi M et al (2018) MRI-targeted or standard biopsy for prostate-cancer diagnosis. N Engl J Med 378(19):1767–1777
van der Leest M, Cornel E, Israël B et al (2019) Head-to-head comparison of transrectal ultrasound-guided prostate biopsy versus multiparametric prostate resonance imaging with subsequent magnetic resonance-guided biopsy in biopsy-naïve men with elevated prostate-specific antigen: a large prospective multicenter clinical study. Eur Urol 75(4):570–578
Mottet N, van den Bergh RCN, Briers E et al (2021) EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer-2020 update part 1 screening, diagnosis and local treatment with curative intent. Eur Urol 79(2):243–262
Tosoian JJ, Mamawala M, Epstein JI, Landis P, Macura KJ, Simopoulos DN, Carter HB, Gorin MA (2020) Active surveillance of grade group 1 prostate cancer: long-term outcomes from a large prospective cohort. Eur Urol 77(6):675–682
Vince RA Jr, Sun Y, Mahal B et al (2022) The impact of a statewide active surveillance initiative: a roadmap for increasing active surveillance utilization nationwide. Eur Urol S0302–2838(22):02405–02408
Eggener SE, Berlin A, Vickers AJ, Paner GP, Wolinsky H, Cooperberg MR (2022) Low-grade prostate cancer time to stop calling it cancer. J Clin Oncol 18:2200123
Epstein JI, Feng Z, Trock BJ, Pierorazio PM (2012) Upgrading and downgrading of prostate cancer from biopsy to radical prostatectomy: incidence and predictive factors using the modified Gleason grading system and factoring in tertiary grades. Eur Urol 61(5):1019–1024
Weinreb JC, Barentsz JO, Choyke PL et al (2016) PI-RADS prostate imaging—reporting and data system: 2015, version 2. Eur Urol 69(1):16–40
Barentsz JO, Richenberg J, Clements R et al (2012) ESUR prostate MR guidelines 2012. Eur Radiol 22(4):746–757
Thaxton CS, Loeb S, Roehl KA, Kan D, Catalona WJ (2010) Treatment outcomes of radical prostatectomy in potential candidates for 3 published active surveillance protocols. Urology 75(2):414–418
Kovac E, Vertosick EA, Sjoberg DD, Vickers AJ, Stephenson AJ (2018) Effects of pathological upstaging or upgrading on metastasis and cancer-specific mortality in men with clinical low-risk prostate cancer. BJU Int 122(6):1003–1009
Lantz A, Falagario UG, Ratnani P et al (2022) Expanding active surveillance inclusion criteria: a novel nomogram including preoperative clinical parameters and magnetic resonance imaging findings. Eur Urol Oncol 5(2):187–194
Sanda MG, Dunn RL, Michalski J et al (2008) Quality of life and satisfaction with outcome among prostate-cancer survivors. N Engl J Med 358(12):1250–1261
Press BH, Jones T, Olawoyin O et al (2022) Association between a 22-feature genomic classifier and biopsy gleason upgrade during active surveillance for prostate cancer. Eur Urol Open Sci 11(37):113–119
Jairath NK, Dal Pra A, Vince R Jr et al (2021) A systematic review of the evidence for the decipher genomic classifier in prostate cancer. Eur Urol 79(3):374–383
Banerjee PS (2022) A review on the role of tissue-based molecular biomarkers for active surveillance. World J Urol 40(1):27–34
Eggener SE, Rumble RB, Armstrong AJ et al (2020) Molecular biomarkers in localized prostate cancer ASCO guideline. J Clin Oncol 38(13):1474–1494
Carter HB, Partin AW, Walsh PC et al (2012) Gleason score 6 adenocarcinoma: should it be labeled as cancer? J Clin Oncol 30(35):4294–4296
Tzeng M, Basourakos SP, Davuluri M, Nagar H, Ramaswamy A, Cheng E, DeMeo G, Jim CHU (2022) Evolving trends in the management of low-risk prostate cancer. Clin Genitourin Cancer. https://doi.org/10.1016/j.clgc.2022.05.004
Epstein JI (2022) Is grade group 1 (Gleason score 3 + 3 = 6) adenocarcinoma of the prostate really cancer? Curr Opin Urol 32(1):91–95
Desai MM, Cacciamani GE, Gill K et al (2022) Trends in incidence of metastatic prostate cancer in the US. JAMA Netw Open 5(3):e222246
Funding
The study was not funded.
Author information
Authors and Affiliations
Consortia
Contributions
Study concept and design: BP. Acquisition of data: MR, AP, MO, EB, GF, DF, ALC, GT, DL, PVC, MR, RD, PD, AT, JBB, AR, Ploussard. Analysis and interpretation of data: Baboudjian, Roumiguié, Peltier, Oderda, Barret, Fromont, CD, Fiard, ALC, GT, DL, VC, MR, RD, PD, AT, JBB, LD, MR, MR, GP. Drafting of the manuscript: MB, GP. Critical revision of the manuscript for important intellectual content: TR, PD, MO, EB, GF, CD, GF, MR, RD, Diana, JB, PD, MR, AR. Statistical analysis: GT.
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflict of interest.
Ethical approval
All procedures performed in this study were approved with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.\
Consent to participate
Patient consent was not required due to the study design (retrospective).
Consent for publication
All authors approve the submission.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Baboudjian, M., Roumiguié, M., Peltier, A. et al. Grade group 1 prostate cancer on biopsy: are we still missing aggressive disease in the era of image-directed therapy?. World J Urol 40, 2423–2429 (2022). https://doi.org/10.1007/s00345-022-04130-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-022-04130-z