
Abstract
Objectives
Liver Imaging Reporting and Data System (LI-RADS) for hepatocellular carcinoma (HCC) diagnosis in high-risk patients is a dynamic system, which was lastly updated in 2018. We aimed to evaluate the accuracy for HCC diagnosis of LI-RADS v2018 with magnetic resonance imaging (MRI) with extracellular contrast for solitary nodules ≤ 20 mm detected during ultrasound (US) surveillance in cirrhotic patients, with particular interest in those observations categorized as LI-RADS 3.
Methods
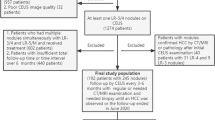
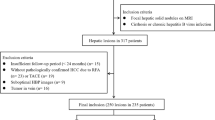
Between November 2003 and February 2017, we included 262 consecutive cirrhotic patients with a newly US-detected solitary ≤ 20-mm nodule. A LI-RADS (LR) v2018 category was retrospectively assigned. The diagnostic accuracy for each LR category was described, and the main MRI findings associated with HCC diagnosis were analyzed.
Results
Final diagnoses were as follows: 197 HCC (75.2%), 5 cholangiocarcinoma (1.9%), 2 metastasis (0.8%), and 58 benign lesions (22.1%); 0/15 (0%) LR-1, 6/26 (23.1%) LR-2, 51/74 (68.9%) LR-3, 11/12 (91.7%) LR-4, 126/127 (99.2%) LR-5, and 3/8 (37.5%) LR-M were HCC. LR-5 category displayed a sensitivity and specificity of 64% (95% CI, 56.8–70.7) and 98.5% (95% CI, 91.7–100), respectively. Considering also LR-4 as diagnostic for HCC, the sensitivity slightly increased to 69.5% (95% CI, 62.6–75.9) with minor impact on specificity (96.2%; 95% CI, 89.3–99.6). Regarding LR-3 observations, 51 out of 74 were HCC, 2 were non-HCC malignancies, and 20 out of 21 LR-3 nodules > 15 mm (95.2%) were finally categorized as HCC.
Conclusions
The high probability of HCC in US-detected LR-3 observations (68.9%) justifies triggering an active diagnostic work-up if intended to diagnose HCC at a very early stage.
Key Points
• In cirrhotic patients with nodules ≤ 20 mm detected during US surveillance, 51 out of 74 (68.9%) of LR-3 nodules by MRI corresponded to an HCC.
• In LR-3 nodules, HCC diagnosis was closely related to baseline tumor size. All 5 nodules smaller than 1 cm were diagnosed as benign. Oppositely, 20 out of 21 LR-3 observations > 15 mm (95.2%) were diagnosed as HCC.
• The high probability of HCC in US-detected LR-3 observations justifies triggering an active diagnostic work-up if intended to diagnose HCC at a very early stage.


Similar content being viewed by others

Abbreviations
- AASLD:
-
American Association for the Study of Liver Diseases
- ACR:
-
American College of Radiology
- CT:
-
Computed tomography
- EASL:
-
European Association for the Study of the Liver
- FNB:
-
Fine-needle biopsy
- HCC:
-
Hepatocellular carcinoma
- iCCA:
-
Intrahepatic cholangiocarcinoma
- LI-RADS/LR:
-
Liver Imaging Reporting and Data System
- MRI:
-
Magnetic resonance imaging
- NAFLD:
-
Non-alcoholic fatty liver disease
- US:
-
Ultrasonography
References
Alazawi W, Cunningham M, Dearden J, Foster GR (2010) Systematic review: outcome of compensated cirrhosis due to chronic hepatitis C infection. Aliment Pharmacol Ther 32:344–355. APT4370. https://doi.org/10.1111/j.1365-2036.2010.04370.x
Galle PR, Forner A, Llovet JM et al (2018) EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 69:182–236. https://doi.org/10.1016/j.jhep.2018.03.019
Heimbach JK, Kulik LM, Finn RS et al (2018) AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 67:358–380. https://doi.org/10.1002/hep.29086
Elsayes KM, Kielar AZ, Agrons MM et al (2017) Liver Imaging Reporting and Data System: an expert consensus statement. J Hepatocell Carcinoma 4:29–39. https://doi.org/10.2147/JHC.S125396
Darnell A, Forner A, Rimola J et al (2015) Liver Imaging Reporting and Data System with MR imaging: evaluation in nodules 20 mm or smaller detected in cirrhosis at screening US. Radiology 275:698–707. https://doi.org/10.1148/radiol.15141132
Choi J-Y, Cho HC, Sun M et al (2013) Indeterminate observations (liver imaging reporting and data system category 3) on MRI in the cirrhotic liver: fate and clinical implications. AJR Am J Roentgenol 201:993–1001. https://doi.org/10.2214/AJR.12.10007
Tanabe M, Kanki A, Wolfson T et al (2016) Imaging Outcomes of Liver Imaging Reporting and Data System version 2014 category 2, 3, and 4 observations detected at CT and MR imaging. Radiology 281:129–139. https://doi.org/10.1148/radiol.2016152173
Liu W, Qin J, Guo R et al (2018) Accuracy of the diagnostic evaluation of hepatocellular carcinoma with LI-RADS. Acta Radiol 59:140–146. https://doi.org/10.1177/0284185117716700
Kierans AS, Makkar J, Guniganti P et al (2018) Validation of Liver Imaging Reporting and Data System 2017 (LI-RADS) criteria for imaging diagnosis of hepatocellular carcinoma. J Magn Reson Imaging. https://doi.org/10.1002/jmri.26329
American College of Radiology. Liver Imaging Reporting and Data System version 2018. Accessed March 12 2020, from https://www.acr.org/-/media/ACR/Files/RADS/LI-RADS/LI-RADS-2018-Core.pdf?la=en
Chernyak V, Fowler KJ, Kamaya A et al (2018) Liver Imaging Reporting and Data System (LI-RADS) version 2018: imaging of hepatocellular carcinoma in at-risk patients. Radiology 289:816–830. https://doi.org/10.1148/radiol.2018181494
Forner A, Vilana R, Ayuso C et al (2008) Diagnosis of hepatic nodules 20 mm or smaller in cirrhosis: prospective validation of the noninvasive diagnostic criteria for hepatocellular carcinoma. Hepatology 47:97–104. https://doi.org/10.1002/hep.21966
Khalili KT, Kim TK, Jang HJ et al (2011) Optimization of imaging diagnosis of 1-2 cm hepatocellular carcinoma: an analysis of diagnostic performance and resource utilization. J Hepatol 54:723–728. https://doi.org/10.1016/j.jhep.2010.07.025
Sangiovanni A, Manini MA, Iavarone M et al (2010) The diagnostic and economic impact of contrast imaging technique in the diagnosis of small hepatocellular carcinoma in cirrhosis. Gut 59:638–644. https://doi.org/10.1136/gut.2009.187286
International Consensus Group for Hepatocellular NeoplasiaThe International Consensus Group for Hepatocellular Neoplasia (2009) Pathologic diagnosis of early hepatocellular carcinoma: a report of the international consensus group for hepatocellular neoplasia. Hepatology 49:658–664. https://doi.org/10.1002/hep.22709
Abd Alkhalik Basha M, Abd El Aziz El Sammak D, El Sammak AA (2017) Diagnostic efficacy of the Liver Imaging-Reporting and Data System (LI-RADS) with CT imaging in categorising small nodules (10–20 mm) detected in the cirrhotic liver at screening ultrasound. Clin Radiol 72:901.e1–901.e11. https://doi.org/10.1016/j.crad.2017.05.019
Basha MAA, AlAzzazy MZ, Ahmed AF et al (2018) Does a combined CT and MRI protocol enhance the diagnostic efficacy of LI-RADS in the categorization of hepatic observations? A prospective comparative study. Eur Radiol 28:2592–2603. https://doi.org/10.1007/s00330-017-5232-y
van der Pol CB, Lim CS, Sirlin CB et al (2019) Accuracy of the Liver Imaging Reporting and Data System in computed tomography and magnetic resonance image analysis of hepatocellular carcinoma or overall malignancy—a systematic review. Gastroenterology 156:976–986. https://doi.org/10.1053/j.gastro.2018.11.020
Willatt JM, Hussain HK, Adusumilli S, Marrero JA (2008) MR imaging of hepatocellular carcinoma in the cirrhotic liver: challenges and controversies. Radiology 247:311–330
Khan AS, Hussain HK, Johnson TD et al (2010) Value of delayed hypointensity and delayed enhancing rim in magnetic resonance imaging diagnosis of small hepatocellular carcinoma in the cirrhotic liver. J Magn Reson Imaging 32:360–366. https://doi.org/10.1002/jmri.22271
Kim TK, Lee KH, Jang HJ et al (2011) Analysis of gadobenate dimeglumine-enhanced MR findings for characterizing small (1-2-cm) hepatic nodules in patients at high risk for hepatocellular carcinoma. Radiology 259:730–738. https://doi.org/10.1148/radiol.11101549
Roskams T, Kojiro M (2010) Pathology of early hepatocellular carcinoma: conventional and molecular diagnosis. Semin Liver Dis 30:17–25. https://doi.org/10.1055/s-0030-1247129
Bruix J, Ayuso C (2019) Diagnosis of hepatic nodules in patients at risk for hepatocellular carcinoma: LIRADS probability vs certainty. Gastroenterology 156:860–862. https://doi.org/10.1053/j.gastro.2019.02.008
Kielar AZ, Chernyak V, Bashir MR et al (2019) An update for LI-RADS: version 2018. Why so soon after version 2017? J Magn Reson Imaging 50:1990–1991. https://doi.org/10.1002/jmri.26715
Leoni S, Piscaglia F, Golfieri R et al (2010) The impact of vascular and nonvascular findings on the noninvasive diagnosis of small hepatocellular carcinoma based on the EASL and AASLD criteria. Am J Gastroenterol 105:599–609. https://doi.org/10.1038/ajg.2009.654
Kim SE, Lee HC, Shim JH et al (2011) Noninvasive diagnostic criteria for hepatocellular carcinoma in hepatic masses larger than 2 cm in a hepatitis B virus-endemic area. Liver Int 31:1468–1476. https://doi.org/10.1111/j.1478-3231.2011.02529.x
Erkan B, Meier J, Clark TJ et al (2019) Non-invasive diagnostic criteria of hepatocellular carcinoma: comparison of diagnostic accuracy of updated LI-RADS with clinical practice guidelines of OPTN-UNOS, AASLD, NCCN, EASL-EORTC, and KLSCG-NCC. PLoS One 14:e0226291. https://doi.org/10.1371/journal.pone.0226291
Davenport MS, Khalatbari S, Liu PSC et al (2014) Repeatability of diagnostic features and scoring systems for hepatocellular carcinoma by using MR imaging. Radiology 272:132–142. https://doi.org/10.1148/radiol.14131963
Cerny M, Chernyak V, Olivié D et al (2018) LI-RADS version 2018 ancillary features at MRI. Radiographics 38:1973–2001. https://doi.org/10.1148/rg.2018180052
Kang JH, Choi SH, Byun JH et al (2020) Ancillary features in the Liver Imaging Reporting and Data System: how to improve diagnosis of hepatocellular carcinoma ≤ 3 cm on magnetic resonance imaging. Eur Radiol. https://doi.org/10.1007/s00330-019-06645-3
Acknowledgments
Álvaro Díaz-González: Grant support from the Instituto de Salud Carlos III (CM15/00050) and Ayuda Clínico Junior 2018 from the Asociación Española Contra el Cáncer (AECC).
María Reig: Grant support from Instituto de Salud Carlos III (PI15/00145 and PI18/00358).
Jordi Bruix: Grant support from Instituto de Salud Carlos III (PI14/00962 and PI18/00768), AECC (PI044031), Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement (2014 SGR 605), and WCR (AICR) 16-0026.
Alejandro Forner: Grant support from Instituto de Salud Carlos III (PI13/01229 and PI18/00542).
CIBERehd is funded by the Instituto de Salud Carlos III.
Funding
This study has received funding by Instituto de Salud Carlos III (PI18/00542).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Alejandro Forner.
Conflict of interest
The authors of this manuscript declare relationships with the following companies:
Anna Darnell, Álvaro Díaz-González, and Carmen Ayuso: Speaker fees and travel grants from Bayer.
Jordi Rimola: Speaker fees and travel grants from Bayer. Consultancy fees COR2ED.
Ernest Belmonte: Travel grants from BTG.
Enric Ripoll, Carla Caparroz, and Ramón Vilana: None.
Ángeles García-Criado: Speaker fees from BTG and Terumo.
María Reig: Consultancy from Bayer, BMS, Roche, Ipsen, AstraZeneca, and Lilly. Lecture fees from Bayer, BTG, BMS, Gilead, and Lilly. Research grants from Bayer and Lilly.
Jordi Bruix: Consultancy from Arqule, Bayer, Novartis, BMS, BTG-Biocompatibles, Eisai, Kowa, Terumo, Gilead, Bio-Alliance, Roche, AbbVie, Merck, Sirtex, Ipsen, Astra-Medimmune, Incyte, Quirem, Adaptimmune, and Lilly. Research grants from Bayer and BTG. Educational grants from Bayer and BTG. Lecture fees from Bayer, BTG-Biocompatibles, Eisai, Terumo, Sirtex, and Ipsen.
Alejandro Forner: Speaker fees from Bayer, Gilead, and MSD; consultancy fees from Bayer, AstraZeneca, and Guerbert.
None of those declared company relationships are related to the subject matter of the article.
Statistics and biometry
No complex statistical methods were necessary for this paper. Noteworthy, the corresponding author of this article (Alejandro Forner) has a degree on Investigation Methodology in Health Science and a Master in Methodology of Investigation in Health Science by the Universidad Autónoma de Barcelona, Spain.
Informed consent
Written informed consent was waived by the institutional review board.
Ethical approval
Institutional review board approval was obtained.
Study subjects or cohorts overlap
Part of the population study was previously reported to validate the non-invasive diagnostic criteria for hepatocellular carcinoma (Forner A et al Hepatology 2008; 47:97–104), the limited value of intratumoral fat or peritumoral capsule to increase the diagnostic accuracy of MRI (Rimola J et al Journal of Hepatology 2012;56:1317–1323), and the evaluation of the diagnostic accuracy of LI-RADS v2013 (Darnell A et al Radiology. 2015;275:698–707). However, the results of the present study and the previous do not overlap and do not contain redundant information. In particular, the latter study in 2015 by Darnell et al included 133 patients and the lesions were evaluated according to LI-RADS v2013. In the present study, we included 129 additional patients, and the LI-RADS assessment was done with v2018.
Methodology
• Retrospective analysis of a prospective protocol
• Diagnostic or prognostic study
• Performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 26 kb)
Rights and permissions
About this article

Cite this article
Darnell, A., Rimola, J., Belmonte, E. et al. Evaluation of LI-RADS 3 category by magnetic resonance in US-detected nodules ≤ 2 cm in cirrhotic patients. Eur Radiol 31, 4794–4803 (2021). https://doi.org/10.1007/s00330-020-07457-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-020-07457-6