
Abstract
Objectives
The purposes of the study were to evaluate the safety and long-term efficacy of augmented vertebroplasty using a polyether ether ketone (PEEK) implant, for the treatment of lumbar or thoracic vertebral fractures (A2 according to the Magerl’s AO classification) and to analyze pain reduction, height restoration, and complications during a 2-year follow-up period.
Methods
Prospective non-randomized evaluation was performed for 21 painful split vertebral fractures (20 patients, 14 females, 6 males; mean age 72.80 ± 10.991) treated with percutaneous vertebral augmentation using a PEEK device, under fluoroscopic guidance. Pain before the procedure and after 6, 12, and 24 months was evaluated using a numeric visual scale (NVS) questionnaire. Imaging was performed by CT and X-rays. The minimum craniocaudal diameter at the level of the fracture and the maximum craniocaudal diameter at the middle of the fractured vertebra were measured. Statistical analysis was performed to evaluate pain decrease and height restoration.
Results
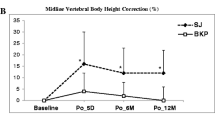
Successful implant positioning was achieved in all cases. No major clinical complications were observed. Comparing the mean pain scores at baseline (8.69 ± 1.138) and the first day after the treatment (1.19 ± 1.424), there was a decrease of 7.50 NVS units (p < 0.001). Minimum and maximum vertebral body heights were increased after the procedure 56.58% and 13.7% respectively (p < 0.001). Both pain relief and height restoration remained statistically significant (p < 0.001) during the follow-up period.
Conclusion
A2 Magerl thoracic or lumbar fractures could be successfully treated with PEEK implant-assisted vertebral augmentation. Randomized studies with larger sample sizes should be done to confirm the effectiveness of the technique.
Key Points
• Vertebral augmentation using a PEEK implant for the treatment of A2 Magerl lumbar or thoracic vertebral fractures seems to be effective both in terms of pain reduction and height restoration.
• Effects on pain reduction and height restoration have a long-term duration.
• The technique seems to be safe for the treatment of A2 Magerl fractures, without major complications in our study group.




Similar content being viewed by others


Abbreviations
- NVS:
-
Numeric visual scale
- PEEK:
-
Polyether ether ketone
- PMMA:
-
Polymethylmethacrylate
- STIR:
-
Short-TI inversion recovery
References
Barr JD, Jensen ME, Hirsch JA et al (2014) Position statement on percutaneous vertebral augmentation: a consensus statement developed by the Society of Interventional Radiology (SIR), American Association of Neurological Surgeons (AANS) and the Congress of Neurological Surgeons (CNS), American College of Radiology (ACR), American Society of Neuroradiology (ASNR), American Society of Spine Radiology (ASSR), Canadian Interventional Radiology Association (CIRA), and the Society of NeuroInterventional Surgery (SNIS). J Vasc Interv Radiol 25(2):171–181
Clark W, Bird P, Gonski P et al (2016) Safety and efficacy of vertebroplasty for acute painful osteoporotic fractures (VAPOUR): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet 388(10052):1408–1416
Santiago FR, Kelekis A, Alvarez LG, Filippiadis DK (2014) Interventional procedures of the spine. Semin Musculoskelet Radiol 18(3):309–317
Tsoumakidou G, Too CW, Koch G et al (2017) CIRSE guidelines on percutaneous vertebral augmentation. Cardiovasc Intervent Radiol 40(3):331–342
Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S (1994) A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 3(4):184–201
Aebi M (2010) Classification of thoracolumbar fractures and dislocations. Eur Spine J 19(1):2–7
De Boeck H, Opdecam P (1999) Split coronal fractures of the lumbar spine. Treatment by posterior internal fixation and transpedicular bone grafting. Int Orthop 23(2):87–90
Kim BG, Dan JM, Shin DE (2015) Treatment of thoracolumbar fracture. Asian Spine J 9(1):133–146
Jutte PC, Castelein RM (2002) Complications of pedicle screws in lumbar and lumbosacral fusions in 105 consecutive primary operations. Eur Spine J 11(6):594–598
Huwart L, Foti P, Andreani O et al (2014) Vertebral split fractures: technical feasibility of percutaneous vertebroplasty. Eur J Radiol 83(1):173–178
Amoretti N, Huwart L (2014) Combination of percutaneous osteosynthesis and vertebroplasty of thoracolumbar split fractures under CT and fluoroscopy guidance: a new technique. Cardiovasc Intervent Radiol 37(5):1363–1368
Fürderer S, Schnurr C, König D (2010) Minimal invasive transvertebral reduction and stabilisation of coronal split fractures. The Internet Journal of Minimally Invasive Spinal Technology 4:1 Available via http://ispub.com/IJMIST/4/1/9250. Accessed 5 Oct 2018
Korovessis P, Vardakastanis K, Repantis T, Vitsas V (2013) Balloon kyphoplasty versus KIVA vertebral augmentation—comparison of 2 techniques for osteoporotic vertebral body fractures. Spine (Phila Pa 1976) 38(4):292–299
Tutton SM, Pflugmacher R, Davidian M, Beall DP, Facchini FR, Garfin SR (2015) KAST study: the Kiva system as a vertebral augmentation treatment—a safety and effectiveness trial: a randomized, noninferiority trial comparing the Kiva system with balloon kyphoplasty in treatment of osteoporotic vertebral compression fractures. Spine (Phila Pa 1976) 40(12):865–875
Mailli L, Filippiadis DK, Brountzos EN, Alexopoulou E, Kelekis N, Kelekis A (2013) Clinical outcome and safety of multilevel vertebroplasty: clinical experience and results. Cardiovasc Intervent Radiol 36(1):183–191
Bonnard E, Foti P, Kastler A, Amoretti N (2017) Percutaneous vertebroplasty under local anaesthesia: feasibility regarding patients’ experience. Eur Radiol 27(4):1512–1516
Kelekis AD, Somon T, Yilmaz H et al (2005) Interventional spine procedures. Eur J Radiol 55(3):362–383
Filippiadis DK, Binkert C, Pellerin O, Hoffmann RT, Krajina A, Pereira PL (2017) Cirse quality assurance document and standards for classification of complications: the Cirse classification system. Cardiovasc Intervent Radiol 40(8):1141–1146
Otten LA, Bornemnn R, Jansen TR et al (2013) Comparison of balloon kyphoplasty with the new Kiva® VCF system for the treatment of vertebral compression fractures. Pain Physician 16(5):505–512
Olivarez LM, Dipp JM, Escamilla RF et al (2011) Vertebral augmentation treatment of painful osteoporotic compression fractures with the Kiva VCF Treatment System. SAS J 5(1):114–119
Anselmetti GC, Manca A, Tutton S et al (2013) Percutaneous vertebral augmentation assisted by PEEK implant in painful osteolytic vertebral metastasis involving the vertebral wall: experience on 40 patients. Pain Physician 16(4):397–404
Heo DH, Chin DK, Yoon YS, Kuh SU (2009) Recollapse of previous vertebral compression fracture after percutaneous vertebroplasty. Osteoporos Int 20(3):473–480
Kim YY, Rhyu KW (2010) Recompression of vertebral body after balloon kyphoplasty for osteoporotic vertebral compression fracture. Eur Spine J 19(11):1907–1912
Beall DP, Olan WJ, Kakad P, Li Q, Hornberger J (2015) Economic analysis of Kiva VCF treatment system compared to balloon kyphoplasty using randomized Kiva Safety and Effectiveness Trial (KAST) data. Pain Physician 18(3):299–306
Anselmetti GC, Manca A, Marcia S et al (2014) Vertebral augmentation with nitinol endoprosthesis: clinical experience in 40 patients with 1-year follow-up. Cardiovasc Intervent Radiol 37(1):193–202
Vanni D, Pantalone A, Bigossi F, Pineto F, Lucantoni D, Salini V (2012) New perspective for third generation percutaneous vertebral augmentation procedures: preliminary results at 12 months. J Craniovertebr Junction Spine 3(2):47–51
Premat K, Vande Perre S, Cormier É et al (2018) Vertebral augmentation with the SpineJack® in chronic vertebral compression fractures with major kyphosis. Eur Radiol. https://doi.org/10.1007/s00330-018-5544-6
Vanni D, Galzio R, Kazakova A et al (2016) Third-generation percutaneous vertebral augmentation systems. J Spine Surg 2(1):13–20
Komemushi A, Tanigawa N, Kariya S et al (2006) Percutaneous vertebroplasty for osteoporotic compression fracture: multivariate study of predictors of new vertebral body fracture. Cardiovasc Intervent Radiol 29(4):580–585
Khosla A, Diehn FE, Rad AE, Kallmes DF (2012) Neither subendplate cement deposition nor cement leakage into the disk space during vertebroplasty significantly affects patient outcomes. Radiology 264(1):180–186
Amoretti N (2018) Early percutaneous vertebroplasty helps motorsport professionals to resume competition soon after vertebral fracture. Eur Radiol 28(7):2870–2871
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Alexios Kelekis.
Conflict of interest
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and biometry
No complex statistical methods were necessary for this paper. One of the authors has significant statistical expertise.
Informed consent
Written informed consent was obtained from all subjects (patients) in this study.
Ethical approval
Institutional review board approval was obtained.
Methodology
• Prospective
• Observational
• Performed at one institution
Rights and permissions
About this article

Cite this article
Velonakis, G., Filippiadis, D., Spiliopoulos, S. et al. Evaluation of pain reduction and height restoration post vertebral augmentation using a polyether ether ketone (PEEK) polymer implant for the treatment of split (Magerl A2) vertebral fractures: a prospective, long-term, non-randomized study. Eur Radiol 29, 4050–4057 (2019). https://doi.org/10.1007/s00330-018-5867-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-018-5867-3