
Abstract
Objectives
To compare a low-tube-voltage with or without high-iodine-load multidetector CT (MDCT) protocol with a normal-tube-voltage, normal-iodine-load (standard) protocol in patients with pancreatic ductal adenocarcinoma (PDAC) with respect to tumour conspicuity and image quality.
Methods
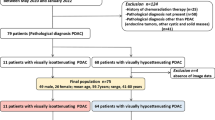
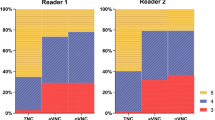
Thirty consecutive patients (mean age: 66 years, men/women: 14/16) preoperatively underwent triple-phase 64-channel MDCT examinations twice according to: (i) 120-kV standard protocol (PS; 0.75 g iodine (I)/kg body weight, n = 30) and (ii) 80-kV protocol A (PA; 0.75 g I/kg, n = 14) or protocol B (PB; 1 g I/kg, n = 16). Two independent readers evaluated tumour delineation and image quality blindly for all protocols. A third reader estimated the pancreas-to-tumour contrast-to-noise ratio (CNR). Statistical analysis was performed with the Chi-square test.
Results
Tumour delineation was significantly better in PB and PA compared with PS (P = 0.02). The evaluation of image quality was similar for the three protocols (all, P > 0.05). The highest CNR was observed with PB and was significantly better compared to PA (P = 0.02) and PS (P = 0.0002).
Conclusion
In patients with PDAC, a low-tube-voltage, high-iodine-load protocol improves tumour delineation and CNR leading to higher tumour conspicuity compared to standard protocol MDCT.
Key Points
• Low-tube-voltage high-iodine-load MDCT improves pancreatic cancer conspicuity compared to a standard protocol.
• The pancreas-to-tumour attenuation difference increases significantly by reducing the tube voltage.
• The radiation exposure dose decreases by reducing the tube voltage.


Similar content being viewed by others

Abbreviations
- ANOVA:
-
Analysis of variance
- ATCM:
-
Automatic tube current modulation
- BMI:
-
Body mass index
- CA:
-
Coeliac axis
- CM:
-
Contrast medium
- CNR:
-
Contrast-to-noise ratio
- CTDIvol:
-
Volume dose index CT
- DLP:
-
Dose length product
- ED:
-
Effective dose
- FOM:
-
Figure of merit
- I:
-
Iodine
- kV:
-
Kilovolt
- MDCT:
-
Multidetector computed tomography
- MTB:
-
Multidisciplinary tumour board
- NCP:
-
Non-contrast phase
- PDAC:
-
Pancreatic ductal adenocarcinoma
- PPP:
-
Pancreatic parenchymal phase
- PPV:
-
Positive predictive value
- PVP:
-
Portal venous phase
- ROI:
-
Region of interest
- SD:
-
Standard deviation
References
Malvezzi M, Arfe A, Bertuccio P, Levi F, La Vecchia C, Negri E (2011) European cancer mortality predictions for the year 2011. Ann Oncol 22:947–956
Gillen S, Schuster T, Meyer Zum Buschenfelde C, Friess H, Kleeff J (2010) Preoperative/neoadjuvant therapy in pancreatic cancer: a systematic review and meta-analysis of response and resection percentages. PLoS Med 7, e1000267
McEvoy SH, Lavelle LP, Hoare SM et al (2014) Pancreaticoduodenectomy: expected post-operative anatomy and complications. Br J Radiol 87:20140050
Heinemann V, Haas M, Boeck S (2013) Neoadjuvant treatment of borderline resectable and non-resectable pancreatic cancer. Ann Oncol 24:2484–2492
Balachandran A, Bhosale PR, Charnsangavej C, Tamm EP (2014) Imaging of pancreatic neoplasms. Surg Oncol Clin N Am 23:751–788
de la Santa LG, Retortillo JA, Miguel AC, Klein LM (2014) Radiology of pancreatic neoplasms: An update. World J Gastrointest Oncol 6:330–343
Brennan DD, Zamboni GA, Raptopoulos VD, Kruskal JB (2007) Comprehensive preoperative assessment of pancreatic adenocarcinoma with 64-section volumetric CT. Radiographics 27:1653–1666
Raman SP, Fishman EK (2012) Advances in CT Imaging of GI Malignancies. Gastrointest Cancer Res 5:S4–S9
Diehl SJ, Lehmann KJ, Sadick M, Lachmann R, Georgi M (1998) Pancreatic cancer: value of dual-phase helical CT in assessing resectability. Radiology 206:373–378
Fletcher JG, Wiersema MJ, Farrell MA et al (2003) Pancreatic malignancy: value of arterial, pancreatic, and hepatic phase imaging with multi-detector row CT. Radiology 229:81–90
Kim JH, Park SH, Yu ES et al (2010) Visually isoattenuating pancreatic adenocarcinoma at dynamic-enhanced CT: frequency, clinical and pathologic characteristics, and diagnosis at imaging. Radiology 257:87–96
Tsutomu T, Katsuyoshi I, Naoki K et al (2015) Pancreatic adenocarcinomas without secondary signs on multiphasic multidetector CT: association with clinical and histopathologic features. Eur Radiol. PubMed PMID: 26084602
Schindera ST, Nelson RC, Mukundan S Jr et al (2008) Hypervascular liver tumors: low tube voltage, high tube current multi-detector row CT for enhanced detection--phantom study. Radiology 246:125–132
Heiken JP, Brink JA, McClennan BL, Sagel SS, Crowe TM, Gaines MV (1995) Dynamic incremental CT: effect of volume and concentration of contrast material and patient weight on hepatic enhancement. Radiology 195:353–357
Yamashita Y, Komohara Y, Takahashi M et al (2000) Abdominal helical CT: evaluation of optimal doses of intravenous contrast material--a prospective randomized study. Radiology 216:718–723
Nakayama Y, Awai K, Funama Y et al (2005) Abdominal CT with low tube voltage: preliminary observations about radiation dose, contrast enhancement, image quality, and noise. Radiology 237:945–951
McNulty NJ, Francis IR, Platt JF, Cohan RH, Korobkin M, Gebremariam A (2001) Multi--detector row helical CT of the pancreas: effect of contrast-enhanced multiphasic imaging on enhancement of the pancreas, peripancreatic vasculature, and pancreatic adenocarcinoma. Radiology 220:97–102
Kidoh M, Nakaura T, Nakamura S et al (2013) Low-dose abdominal CT: comparison of low tube voltage with moderate-level iterative reconstruction and standard tube voltage, low tube current with high-level iterative reconstruction. Clin Radiol 68:1008–1015
Birnbaum BA, Hindman N, Lee J, Babb JS (2007) Multi-detector row CT attenuation measurements: assessment of intra- and interscanner variability with an anthropomorphic body CT phantom. Radiology 242:109–119
Mohammed NM, Mahfouz A, Achkar K, Rafie IM, Hajar R (2013) Contrast-induced Nephropathy. Heart Views 14:106–116
Marin D, Nelson RC, Barnhart H et al (2010) Detection of pancreatic tumors, image quality, and radiation dose during the pancreatic parenchymal phase: effect of a low-tube-voltage, high-tube-current CT technique--preliminary results. Radiology 256:450–459
Deak PD, Smal Y, Kalender WA (2010) Multisection CT protocols: sex- and age-specific conversion factors used to determine effective dose from dose-length product. Radiology 257:158–166
Campbell FVC (2013) Pancreatic pathology - a practical approach. Springer, London
Wayne W, Daniel CLC (1995) Biostatistics: A Foundation for Analysis in the Health Sciences, 6th edn. John Wiley & Sons, New York
Montgomery DC (1991) Design and Analysis of Experiments, 3rd edn. John Wiley & Sons, New York
Yeh BM, Shepherd JA, Wang ZJ, Teh HS, Hartman RP, Prevrhal S (2009) Dual-energy and low-kVp CT in the abdomen. AJR Am J Roentgenol 193:47–54
Kim JE, Newman B (2010) Evaluation of a radiation dose reduction strategy for pediatric chest CT. AJR Am J Roentgenol 194:1188–1193
Schueller-Weidekamm C, Schaefer-Prokop CM, Weber M, Herold CJ, Prokop M (2006) CT angiography of pulmonary arteries to detect pulmonary embolism: improvement of vascular enhancement with low kilovoltage settings. Radiology 241:899–907
Holm J, Loizou L, Albiin N, Kartalis N, Leidner B, Sundin A (2012) Low tube voltage CT for improved detection of pancreatic cancer: detection threshold for small, simulated lesions. BMC Med Imaging 12:20
Donahue TR, Isacoff WH, Hines OJ et al (2011) Downstaging chemotherapy and alteration in the classic computed tomography/magnetic resonance imaging signs of vascular involvement in patients with pancreaticobiliary malignant tumors: influence on patient selection for surgery. Arch Surg 146:836–843
Wang Q, Zhao X, Song J et al (2013) The application of automatic tube current modulation (ATCM) on image quality and radiation dose at abdominal computed tomography (CT): A phantom study. J Xray Sci Technol 21:453–464
Szucs-Farkas Z, Verdun FR, von Allmen G, Mini RL, Vock P (2008) Effect of X-ray tube parameters, iodine concentration, and patient size on image quality in pulmonary computed tomography angiography: a chest-phantom-study. Investig Radiol 43:374–381
Acknowledgments
The authors would like to thank the research nurses G. Gagnö and B. Holmberg for their contributions in patient recruitment, the CT technologist N. Jallo and the physicist J. Holm for their contributions in imaging acquisition as well as the biostatistician P. Näsman for his contributions to the statistical analysis. The scientific guarantor of this publication is Nikolaos Kartalis, M.D., Ph.D., Division of Medical Imaging and Technology, Department of Clinical Science, Intervention and Technology (CLINTEC), Karolinska Institutet, Stockholm, Sweden. The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding. Per Näsman kindly provided statistical advice for this manuscript. Institutional Review Board approval was obtained. Written informed consent was obtained from all patients in this study. Methodology: prospective, randomised diagnostic study, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Loizou, L., Albiin, N., Leidner, B. et al. Multidetector CT of pancreatic ductal adenocarcinoma: Effect of tube voltage and iodine load on tumour conspicuity and image quality. Eur Radiol 26, 4021–4029 (2016). https://doi.org/10.1007/s00330-016-4273-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-016-4273-y