
Abstract
Objective
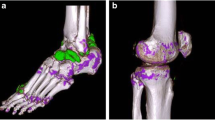
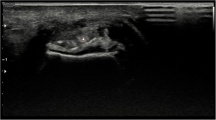
The present study was performed to localize the articular deposition of monosodium urate (MSU) crystal in joints. We compare the detection efficiencies of dual-energy CT (DECT) and ultrasound scans.
Methods
Analyses by DECT and ultrasound were performed with 184 bilateral joints of the lower limbs of 54 consecutive gout patients. All joints were categorized into (1) knee, (2) ankle, (3) MTP1, and (4) MTP2, and sorted into those with and those without detectable MSU deposition. The comparison of the positive rate between DECT and ultrasound and the agreement was performed using the McNemar test and the Cohen’s κ coefficient, respectively. Next, we listed the MSU crystal deposition as assessed by ultrasound between the DECT-positive and -negative joints according to their interior structure. We included tendons, synovia, cartilage, subcutaneous tissue, etc.
Results
Among all joints, the percentages with MSU crystal deposition detected by DECT (99/184, 53.8%) and ultrasound (106/184, 57.6%) were comparable (P = 0.530 > 0.05). For MTP1 (21/34, 61.8%; 12/34, 35.3%; P < 0.05) and MTP2-5 (17/34, 50.0%; 10/34, 29.4%, P < 0.05), ultrasound and DECT were more efficient, respectively. The data concordance in 46 of 50 joints (92.00%; κ = 0.769, P < 0.05) for knee; and 27 of 34 joints (79.41%; κ = 0.588, P < 0.05) for MTP2-5 and suggested that tendons were the most frequent anatomical location of MSU crystal deposition.
Conclusions
The tendons are the most frequent anatomical location of MSU crystal depositions. The concordance rate of knee joints and MTP2-5 joints shows good agreement between DECT and ultrasound depending on the location.






Similar content being viewed by others

References
Hoskison TK, Wortmann RL (2006) Advances in the management of gout and hyperuricaemia. Scand J Rheumatol 35:251–260
Girish G, Melville DM, Kaeley GS et al (2013) Imaging appearances in gout. Arthritis 673401
Dalbeth N, Aati O, Gao A, House M, Liu Q, Horne A et al. (2012) Assessment of tophus size: a comparison between physical measurement methods and dual-energy computed tomography scanning. J Clin Rheumatol 18:23–27
Wallace KL, Riedel AA, Joseph-Ridge N, Wortmann R (2004) Increasing prevalence of gout and hyperuricemia over 10 years among older adults in a managed care population. J Rheumatol 31:1582–1587
Janssens HJEM., Janssen M, van de Lisdonk EH, Fransen J, van Riel PLCM, Weel CV (2009) Limited validity of the American College of Rheumatology criteria for classifying patients with gout in primary care. Ann Rheum Dis 69:1255–1256
Chowalloor PV, Keen HI (2013). A systematic review of ultrasonography in gout and asymptomatic hyperuricaemia. Ann Rheum Dis 72:638–645
Neogi T, Jansen TLTA, Dalbeth N, Vazquez-Mellado J (2016) Gout classification criteria: an American college of rheumatology/European league against rheumatism collaborative initiative. Ann Rheum Dis 67:2557–2568
Thiele RG (2011) Role of ultrasound and other advanced imaging in the diagnosis and management of gout. Curr Rheumatol Rep 13:146–153
Sc SJCB, Chadha Y, Nicolaou S (2010) Dual energy CT: In the detection of monosodium urate in patients with gouty arthropathy. In: Radiological society of North America 2010 scientific assembly and meeting
Wakefield RJ, Brown A, O’Connor P, Grainger A, Karim Z, Mcgonagle D et al (2003) Rheumatological US. Rheumatology 42:1001
Terslev L, Gutierrez M, Schmidt WA, Keen HI, Filippucci E, Kane D et al (2015) Ultrasound as an outcome measure in Gout. A validation process by the OMERACT ultrasound Working Group. J Rheumatol 42:2177–2181
Mallinson PI, Reagan AC, Coupal T, Munk PL, Ouellette H, Nicolaou S (2014) The distribution of urate deposition within the extremities in gout: a review of 148 dual-energy CT cases. Skeletal Radiol 43:277–281
Wallace SL, Robison H, Masi AT, Decker JL, Mccarty DJ, Yu TF (1977) Preliminary criteria for the classification of the acute arthritis of primary gout. Arthritis Rheum 20:895–900
Swan A, Amer H, Dieppe P (2002) The value of synovial fluid assays in the diagnosis of joint disease: a literature survey. Ann Rheum Dis 61:493–498
Zhu L, Wu H, Wu X, Sun W, Zhang T, Ye L et al. (2015) Comparison between dual-energy computed tomography and US in the diagnosis of gout of various joints. Acad Radiol 22:1497–1502
Gruber M, Bodner G, Rath E, Supp G, Weber M, Schuellerweidekamm C (2014) Dual-energy computed tomography compared with US in the diagnosis of gout. Rheumatology 53:173–179
Tanaka R, Hayashi T, Ike M, Noto Y, Goto TK (2013) Reduction of dark-band-like metal artifacts caused by dental implant bodies using hypothetical monoenergetic imaging after dual-energy computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol 115:833–838
Malik A, Schumacher HR, Dinnella JE, Clayburne GM (2009) Clinical diagnostic criteria for gout: comparison with the gold standard of synovial fluid crystal analysis. J Clin Rheumatol 15:22–24
Naredo E, Uson J, Jimenez-Palop M et al (2014) US -detected musculoskeletal urate crystal deposition: which joints and what findings should be assessed for diagnosing gout? Ann Rheum Dis 73:1522–1528
Radice F, Monckeberg JE, Carcuro G (2011) Longitudinal tears of peroneus longus and brevis tendons: a gouty infiltration. J Foot Ankle Surg 50:751–753
Abate M, Schiavone C, Salini V, Andia I (2013) Occurrence of tendon pathologies in metabolic disorders. Rheumatology 52:599–608
Sun N, Zhong S, Li Y, Wu L, Di Y (2016) Urate crystals deposition in the feet of overweight juveniles and those with symptomatic hyperuricemia: a dual-energy CT study. J Pediatr Endocrinol Metab 29:579–583
Dalbeth N, Kalluru R, Aati O, Horne A, Doyle AJ, Mcqueen FM (2013) Tendon involvement in the feet of patients with gout: a dual-energy CT study. Ann Rheum Dis 72:1545–1548
Filippucci E, Delle SA, Riente L, Di GL, Carli L, Ceccarelli F et al (2013) US imaging for the rheumatologist. XLVII. US of the shoulder in patients with gout and calcium pyrophosphate deposition disease. Clin Exp Rheumatol 31:659–664
Konatalapalli RM, Demarco PJ, Jelinek JS et al (2009) Gout in the axial skeleton. J Rheumatol 36:609–613
Funding
The study was funded by the National Natural Science Foundation of China 81273286 and International Collaborative Project in Science and Technology of the Sichuan province 2015HH0050.
Author information
Authors and Affiliations
Contributions
There are nine authors for the original article. The contributions of each author were: (1) The idea of this article was provided by YZ and MH. And YZ is the corresponding author who helped collect patients in the out-patient department. (2) YY was responsible for data collection, processing, drawing, charting, literature review, and article writing. (3) CL, QX and LQ provided specialized guidance of DECT and ultrasound. (4) TY provided rich experience of data collection, processing and article writing for YY. (5) YL, YL, YZ and MH finalized the article. All authors have read and approved this version of the article, and declare no financial or other relationships that could lead to a conflict of interest among authors.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there are no conflicts of interest related to the publication of this paper.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Yuan, Y., Liu, C., Xiang, X. et al. Ultrasound scans and dual energy CT identify tendons as preferred anatomical location of MSU crystal depositions in gouty joints. Rheumatol Int 38, 801–811 (2018). https://doi.org/10.1007/s00296-018-3994-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-018-3994-4