
Abstract
Purpose
To evaluate the feasibility and effectiveness of feeding tube insertion and enteral feeding for the treatment of postoperative gastrointestinal anastomotic obstruction and leakage.
Materials and Methods
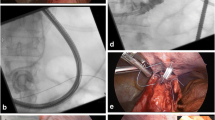
From June 1999 to June 2002, thirty-four cases of postoperative gastrointestinal anastomotic obstruction and leakage after surgery for gastric carcinoma were treated by insertion of a feeding tube under fluoroscopic guidance. Twenty-one patients were male and 13 were female. The patients’ ages ranged from 39 to 74 years (mean age: 61 years). All the patients experienced vomiting, and 15 patients had anastomotic site or duodenal stump leakage. We evaluated the feasibility of feeding tube insertion for enteral feeding to improve the obstruction and facilitate leakage site closure, and the patients’ nutritional benefit was also evaluated by checking the serum albumin level between pre- and post-enteral feeding via the feeding tube.
Results
Thirty-two patients (94%) were successfully managed by feeding tube insertion, but the remaining two were not managed, and this was due to severe angulations at the anastomotic site. The procedure times for feeding tube insertion ranged from 15 to 60 minutes (mean time: 45 minutes). Twenty-eight patients experienced symptomatic relief of gastrointestinal obstruction, and they were able to resume a normal regular diet after feeding tube removal. Three patients underwent stent insertion due to recurrent symptoms, and one patient underwent jejunostomy feeding due to the presence of a persistent leakage site. Eleven patients achieved leakage site closure after enteral feeding via a feeding tube. The serum albumin level was significant, increased from pre-enteral feeding (2.65 ± 0.37 g/dL) to the post-enteral feeding (3.64 ± 0.58 g/dL) via the feeding tube (p < 0.001). The duration of follow-up ranged from one to 53 months (mean: 23 months).
Conclusion
The insertion of a feeding tube for enteral feeding under fluoroscopic guidance is safe, and it provides effective relief from gastrointestinal anastomotic site obstruction and leakage after gastric surgery. Moreover, our findings indicate that feeding tube insertion for enteral feeding may be used as the primary procedure to treat postoperative anastomotic obstruction and leakage.




Similar content being viewed by others


References
Sand J, Luostarinen M, Matikaninen M (1997) Eneteral or parenteral feeding after total gastrectomy: prospective randomised pilot study. Eur J Surg 163:761–766
Papapietro K, Diaz E, Csendes A, et al. (2002) Early enteral nutrition in cancer patients subjected to a total gastrectomy. Rev Med Child 130:1125–1130
Urschel JD, (1995) Esophagogastrostomy anastomotic leaks complicating esophagectomy: a review. Am J Surg 169:634–640
Roy-Choudhury SH, Nicholson AA, Wedgwood KR, et al. (2001) Symptomatic malignant gastroesophageal anastomotic leak: management with covered metallic esophageal stents. Am J Roentgenol 176:161–165
Kwak HS, Lee JM, Jin GY, et al. (2003) Treatment of gastrojejunal anastomotic leak with a covered metallic stent. Hepatogastroenterology 50:62–64
Salo JA, Saario I, Kivilaakso EO, et al. (1988) Near-total gastrectomy for gastric cancer. Am J Surg 155:486–489
Tarazi R, Coutsoftides T, Steiger E, et al. (1983) Gastric and duodenal cutaneous fistulas. World J Surg 7:463–473
Shchepotin IB, Evans SRT, Chorny VA, et al. (1996) Postoperative complications requiring relaparotomies after 700 gastrectomies performed for gastric cancer. Am J Surg 171:270–273
Heindel W, Gossmann A, Fischbach R, et al. (1996) Treatment of a ruptured anastomotic esophageal stricture following bougienage with a Dacron-covered nitinol stent. Cardiovasc Intervent Radiol 19:431–434
Alivizatos V, Felekis D, Zorbalas A (2002) Evaluation of the effectiveness of octreotide in the conservative treatment of postoperative enterocutaneous fistulas. Hepatogastroenterology 49:1010–1012
Ott DJ, Mattox HE, Gelfand DW, et al. (1991) Enteral feeding tubes: placement by using fluoroscopy and endoscopy. Am J Roentgenol 157:769–771
Foote JA, Kemmeter PR, Prichard PA, et al. (2004) A randomized trial of endoscopic and fluoroscopic placement of postpyloric feeding tube in critically ill patients. J Parenter Enteral Nutr 28:154–157
Acknowledgments
The author thanks Bonnie Hami, MA, of the Department of Radiology, University Hospitals of Cleveland for her editorial assistance in the preparation of this article and Kevin Condren of the Harrisco Language Research Institute for his editorial assistance in the revision of the article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Han, YM., Kim, CY., Yang, DH. et al. Fluoroscopically Guided Feeding Tube Insertion for Relief of Postoperative Gastrointestinal Anastomotic Obstruction and Leakage. Cardiovasc Intervent Radiol 29, 395–400 (2006). https://doi.org/10.1007/s00270-005-0095-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-005-0095-z