
Avoid common mistakes on your manuscript.
Level of Evidence V This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
This article entitled “Caudal Septal Extension Graft Sutured with Absorbable Material and Not Fixed to The Nasal Spine Region Compared with The Conventional Fixation Method” surveys a large patient population (1146) operated on by the same surgeon over a 10-year period. Those numbers alone deserve attention on this paper and its contents.
The authors are essentially comparing retrospectively two groups of patients: the first one in which “conventional” methods of fixation of the septal extension graft (SEG) were employed, i.e., end-to-side fixation with permanent sutures (5/0 Prolene) together with nasal spine fixation in some patients, and the second one in which no nasal spine fixation was employed and the same end-to-side suture of SEG was done by absorbable sutures (5/0 Vicryl). The conclusions of the study are that essentially no spine fixation is ever necessary, absorbable sutures have no more complications regarding control of deviation and projection than permanent sutures, and that absorbable are actually advantageous because they diminish the risk of suture-related extrusion. The type of both absorbable and non-absorbable sutures used by the authors is the same used by most rhinoplasty surgeons today.
The first comment is one of terms, and the second one of substance, i.e., contents.
Let’s start with the first, which is briefer than the second.
According to the Cambridge dictionary, the term “conventional” refers essentially to “traditional and ordinary” and “following the usual practices of the past.” This term is liberally used by the authors throughout the whole paper, starting from its very title, as contrasted to the “novel” technique demonstrated and discussed. I would raise an exception on this and its potential implicit meaning: it shouldn’t be a matter of opposing new to old, but of proving the advantages of unproven concepts over well-established ones.
Let’s now briefly scrutinize some issues regarding the contents of the paper.
I certainly agree with the authors on the usefulness of SEG: it is truly one of the most effective techniques for providing precise tip support in open rhinoplasty [1]. This is due to its adjustability and versatility, and obviously even more so in patients with thick skin and weak alar cartilages. It is not strictly necessary to adopt pioneering classifications in the literature [2] to understand that septal extension grafts can be practically fine-tuned in multiple ways, according to the requisites needed on the table for the specific case. This will involve adjusting height, length, projection, and inclination of that specific segment of harvested septum that will be used as an SEG. Finesse in establishing inclination, lengthening and projection of the SEG, and thus precise control in establishing the desired tip position can be achieved by positioning the graft more cranially, more caudally, and shaping it carefully and appropriately. This is an unsurpassed benefit of the SEG, of obvious use in primary rhinoplasties as well as in secondaries, where rib will be often needed for the purpose. Innovative constructs as composite SEGs can also be considered where the cartilaginous septum is in short supply, including a segment of ethmoid plate in continuity with the cartilaginous portion, which will be thinned appropriately, perforated and fixated end-to-side, to the residual septum, with the added bonus of providing further stability to the distal septum.
Having said this, one of the tenets of using an SEG is having a reliably stable caudal residual septum to which the SEG is solidly fixed. Midline stability of the septum is key for structural thinking in rhinoplasty, especially via the open approach. For this reason, a few comments need to be made about the methods and findings of this paper:
-
1.
The choice of end-to-side fixation, as the sole chosen method of stabilization of SEGs, seems logical and can be agreed upon. In my practice, I found the use of figure-of-eight end-to-end fixations, even if variably designed, not equally stable, and prefer to employ a thin ethmoid bone splint as a bridging support when lack of available septum dictates an end-to-end construct.
-
2.
The authors compared the two most representative groups in their experience: patients with SEG fixated with permanent sutures with or without fixation to the spine versus patients with SEG fixated with non-permanent sutures, without any fixation to the spine. This can be disputed for two reasons:
-
(a)
A third group of patients could, and probably should, have been considered in the study: it is common for many surgeons to fixate the SEG to the residual distal septum with absorbable sutures (I liberally use 5/0 dyed PDS on a round needle to this purpose), but a single non-absorbable suture can still frequently be placed to reposition the distal septum or/and the SEG to the septal spine, either using periosteum if available and robust enough, or, preferably, by transosseous suturing. This would logically not pose many issues about suture extrusion: for instance, I’ve been using a 4/0 or 5/0 Prolene (according to requisites) for this maneuver for many years and I have not had a single occurrence of suture extrusion, which can be well understood due to the ample soft tissue pad overlying the stitch, which is cut short with the knot brought to the side of the spine. If one needs further reassurance, a 5/0 Monocryl suture can be used for overlapping periosteum, or soft tissue over the permanent knot.
-
(b)
The authors used nasal spine fixation in “some” of the cases of the first group and, surprisingly, in none of the second. I believe, however, that renouncing to any fixation at the nasal spine can be hazardous and unpredictable. When the distal septum is deviated, notwithstanding the way the deviation is corrected (either scoring and splinting or reconstituting the L-strut from new segments), it will be often logical and necessary to secure it back to the nasal spine [3] (Fig. 1). This both because the septum might be originally dislocated distally from the midline and because the residual L-strut, after septal harvest and/or deviation correction, may become unstable and separated from its attachments to the spine. Resuturing centrally to the spine may also involve modifying the spine itself (e.g., lateral split or central wedge removal) to allow a better fit and transosseous suturing. In the experience of many surgeons, a stabilized caudal septum is thus an essential prerequisite for stabilizing tip symmetry and projection (Fig. 1). Having said this, it remains obvious that in many instances where a SEG is used, the SEG per se does not need to extend down to the nasal spine (Fig. 2), which would happen only in the cases where the distal septum has to be replaced (a “distal septum replacement graft” configuration rather than a “septal extension graft”) or in those relatively few cases in which the septum would have to be lengthened caudally consistently. Thus, resuturing to the spine should often involve only the native septum, in those instances where it has to be brought back to the middle and not the SEG.
Fig. 1 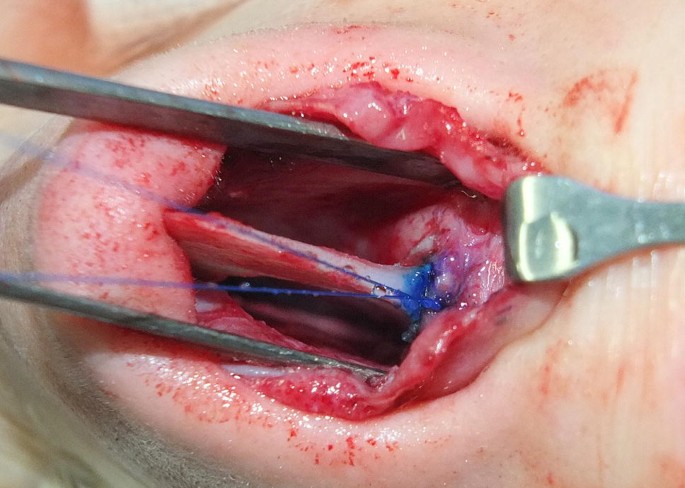
The typical transosseous suture of 4/0 Prolene is demonstrated. The suture will be cut short and will not extrude due to the considerable soft tissue pad overlying it. In some cases, a further 5/0 Monocryl suture can be used to overlay soft tissue or perichondrium over the non-resorbable knot
Fig. 2 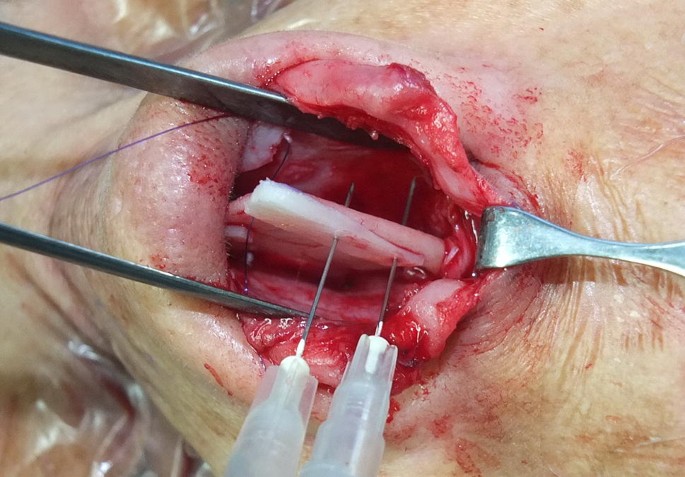
A small SEG is seen positioned to splint and lengthen weak distal septum. The thicker portion of the graft abuts the thinner portion of the cranial distal septum. Fixation will be done with 5/0 dyed PDS interrupted stitches on a round needle. The septum has already been anchored to the nasal spine by a 4/0 transosseous Prolene suture on a round needle
-
(a)


One interesting concept which emerges from the paper and is obviously supported by the authors’ extensive experience is the fact that releasing extrinsic forces from distal septal deviation is the main maneuver to guarantee long-term stability. This is a point that has merit and should be noted: although I personally believe that it may not suffice and that reestablishing midline stability by reanchoring to the nasal spine remains important, it is also true that, oftentimes, fixation techniques become excessive, also causing unneeded further stiffness. Having said this, I don’t consider cartilaginous cross-hatching incisions and other maneuvers alluded to by the authors, and shown to some degree in the photographs accompanying the article, predictable enough to substitute distal septum fixation, even when the dorsal L-strut is stable. Such fixation will only take a minute or two, and a manual sharp awl will be usually enough to pass a suture through the spine.
Essentially, the authors of this paper are to be commended for the numbers of the study and the long-term follow-up, and their results warrant a reflection on avoiding certain maneuvers of fixation in cases where they are not necessary. The division into two groups, although useful to simplify the results, can be, however, questionable, and I would advise readers to be cautious in discarding the time-honored technique of correcting septal deviations distally and stabilizing the straightened segment to the nasal spine. This may take a few minutes but would make me sleep more safely at night.
References
Kim MH, Choi JH, Kim MS, Kim SK, Lee KC (2014) An introduction to the septal extension graft. Arch Plast Surg 41(1):29–34
Byrd HS, Andochick S, Copit S, Walton KG (1997) Septal extension grafts: a method of controlling tip projection shape. Plast Reconstr Surg 100:999
Heppt W, Gubisch W (2011) Septal surgery in rhinoplasty. Facial Plast Surg 27(2):167–178
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declares that he has no conflicts of interest to disclose.
Human and Animal Rights
This article does not contain any studies with human participants or animals performed by the author.
Informed Consent
For this type of study informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Robotti, E. Invited Commentary on Caudal Septal Extension Graft Sutured with Absorbable Material and Not Fixed to the Nasal Spine Region Compared with the Conventional Fixation Method: A Retrospective Study. Aesth Plast Surg 43, 768–770 (2019). https://doi.org/10.1007/s00266-019-01332-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-019-01332-6