
Abstract
Purpose
Infection of a total hip replacement is potentially a devastating complication. Statistical process control methods have been generating interest as a means of improving the quality of healthcare, and we report our experience with the implementation of such a method to monitor the one year infection rate after primary total hip replacement.
Method
Infection was defined as the growth of the same organism in cultures of at least two aspirates or intra-operative specimens, or growth of one pathogen in a patient with local signs of infection such as erythema, abscess or draining sinus tract. The cumulative summation test (CUSUM test) was used to continuously monitor the one year postoperative infection rate. The target performance was 0.5% and the test was set to detect twice that rate.
Results
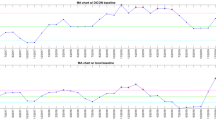
Over the three year study period, 2006 primary total hip replacements were performed. Infection developed within one year after surgery in eight (0.4%) hips. The CUSUM test generated no alarms during the study period, indicating that there was no evidence that the process was out of control.
Conclusion
The one year infection rate after primary total hip replacement was in control. The CUSUM test is a useful method to continuously ensure that performance is maintained at an adequate level.


Similar content being viewed by others


References
Arias KM (2008) Mandatory reporting and pay for performance: health care infections in the limelight. AORN J 87:750–758
Astagneau P, Desplaces N, Vincent V, Chicheportiche V, Botherel A, Maugat S, Lebascle K, Leonard P, Desenclos J, Grosset J, Ziza J, Brucker G (2001) Mycobacterium xenopi spinal infections after discovertebral surgery: investigation and screening of a large outbreak. Lancet 358:747–751
Biau DJ, Milet A, Thevenin F, Anract P, Porcher R (2009) Monitoring surgical performance: an application to total hip replacement. J Eval Clin Pract 15:420–424
Biau DJ, Landreau P, Graveleau N (2010) Monitoring surgical performance: an application of industrial quality process control to anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 18:1263–1268
Biswas P, Kalbfleisch JD (2008) A risk-adjusted CUSUM in continuous time based on the Cox model. Stat Med 27:3382–3406
Berry DJ, Harmsen WS, Cabanela ME, Morrey BF (2002) Twenty-five-year survivorship of two thousand consecutive primary Charnley total hip replacements: factors affecting survivorship of acetabular and femoral components. 84-A:171–177
Biring GS, Kostamp T, Garbuz DS, Masri BA, Duncan CP (2009) Two-stage revision arthroplasty of the hip for infection using an interim articulated Prostalac hip spacer. J Bone Joint Surg Br 91-B:1431–1437
Blom AW, Taylor AH, Pattison G, Whitehouse S, Bannister GC (2003) Infection after total hip arthroplasty. The Avon experience. J Bone Joint Surg Br 85:956–959
Bozic KJ, Kurtz SM, Lau E, Ong K, Vail TP, Berry DJ (2009) The epidemiology of revision total hip arthroplasty in the United States. J Bone Joint Surg Am 91:128–133
The report of the public inquiry into children’s heart surgery at the bristol royal infirmay 1984-1995 (2001) http://www.bristol-inquiry.org.uk/.
de Leval MR, Francois K, Bull C, Brawn W, Spiegelhalter D (1994) Analysis of a cluster of surgical failures. Application to a series of neonatal arterial switch operations. J Thorac Cardiovasc Surg 107:914–923
Fender D, Harper WM, Gregg PJ (1999) Outcome of Charnley total hip replacement across a single health region in England: the results at five years from a regional hip register. J Bone Joint Surg Br 81:577–581
Hardoon SL, Lewsey JD, van der Meulen JH (2007) Continuous monitoring of long-term outcomes with application to hip prostheses. Stat Med 26:5081–5099
Institute of Medicine (2000) To Err Is Human: Building a Safer Health System. National academy press, Washington, DC
Institute of Medicine (2001) Crossing the quality chasm: a new health care system for the 21st century. National academy press, Washington, DC
Jamsen E, Furnes O, Engesaeter LB, Konttinen YT, Odgaard A, Stefansdottir A, Lid-gren L (2010) Prevention of deep infection in joint replacement surgery. Acta Orthop 81:660–666
Klouche S, Sariali E, Mamoudy P (2010) Total hip arthroplasty revision due to infection: a cost analysis approach. Orthop Traumatol Surg Res 96:124–132
Kurtz SM, Ong K, Lau E, Mowat F, Halpern M (2007) Projections of Primary and Revision Hip and Knee Arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am 89:780–785
Learmonth ID, Young C, Rorabeck C (2007) The operation of the century: total hip replacement. Lancet 370:1508–1519
Montgomery DC (2005) Introduction to statistical quality control, 5th edn. John Wiley and Sons, New York
Page ES (1954) Continuous inspection schemes. Biometrika 41:100–115
Park YS, Moon YW, Lim SJ, Oh I, Lim JS (2005) Prognostic factors influencing the functional outcome of total hip arthroplasty for hip infection sequelae. J Arthroplasty 20:608–613
Phillips JE, Crane TP, Noy M, Elliott TS, Grimer RJ (2006) The incidence of deep prosthetic infections in a specialist orthopaedic hospital: a 15-year prospective survey. J Bone Joint Surg Br 88:943–948
Pulido L, Ghanem E, Joshi A, Purtill JJ, Parvizi J (2008) Periprosthetic joint infection: the incidence, timing, and predisposing factors. Clin Orthop Relat Res 466:1710–1715
Romano CL, Romano D, Logoluso N, Meani E (2010) Septic versus aseptic hip revision: how different? J Orthop Traumatol 11:167–174
Schutzer SF, Harris WH (1988) Deep-wound infection after total hip replacement under contemporary aseptic conditions. J Bone Joint Surg Am 70:724–727
Sego LH, Reynolds MR, Woodall WH (2009) Risk-adjusted monitoring of survival times. Stat Med 28:1386–1401
Spiegelhalter D, Grigg O, Kinsman R, Treasure T (2003) Risk-adjusted sequential probability ratio tests: applications to Bristol, Shipman and adult cardiac surgery. Int J Qual Health Care 15:7–13
Tillett HE, Spencer IL (1982) Influenza surveillance in England and Wales using routine statistics. Development of ’cusum’ graphs to compare 12 previous winters and to monitor the 1980/81 winter. J Hyg (Lond) 88:83–94
Wenzel RP (2010) Minimizing surgical-site infections. N Engl J Med 362:75–77
Barbujani G, Calzolari E (1984) Comparison of two statistical techniques for the surveillance of birth defects through a Monte Carlo simulation. Stat Med 3:239–247
Chen R (1987) The relative efficiency of the sets and the cusum techniques in monitoring the occurrence of a rare event. Stat Med 6:517–525
Acknowledgements
We are grateful to Annie Vincensini and Michel Droniou-Cassaro for their dedicated administrative and IT help.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
The CUSUM test1 (cumulative summation test) was used to monitor the infection rate after primary total hip replacement (THR). The CUSUM sequentially tests after each observation X t (t > 0) the following hypothesis H0: λ = λ0, i.e. the process is in control, versus H1: λ≠ λ0, i.e. the process is out of control. The value λ0 is referred to as the target infection rate in this report. The test is based on the statistic S t computed after each observation X t as:
where the sample weight W t depends on the observation X t , λ0, and rate ratio (RR) (see Eq. 2). The test statistic S t is compared with a predefined limit, h. If S t equals or exceeds h, the null hypothesis is rejected. In quality control wording, the CUSUM test is said to emit an alarm indicating that the process is out of control. As long as S t remains below h, the null hypothesis cannot be rejected, and monitoring continues under the assumption that the process is in control. In this report, a CUSUM for time to event data based on a Poisson distribution was chosen, with the following sample weight:
where O j represents the number of THR infection observed on interval j, E j (see Eq. 3) represents the number of THR infection expected on interval j under the null hypothesis of an infection rate of λ0, and RR represents the rate ratio defining the smallest unacceptable increase in the infection rate relative to the target that one wants to detect.
E j is defined as:
where t i is the length of time that a patient i remains infection free during the interval before censoring.
The CUSUM test has a particular feature: it has a holding barrier at zero and can never accept the null hypothesis. Therefore, theoretically, regardless the true performance of the process under observation, type I and type II errors of the test are 100% and 0%, respectively, and performances of CUSUM tests are expressed differently, namely, with the true and false discovery rates (TDR and FDR). These rates correspond to the probability of an alarm to be emitted under the alternative and null hypotheses, respectively, within a defined number of observations2. Also, because of that holding barrier at 0, the score S t cannot deviate too far from the decision limit over long periods without any infection, and it remains responsive at all times to a sudden increase in the infection rate.
In our study, the target infection rate (process in control) chosen was λ0 = 0.5%, and the RR to detect was two; the out-of-control infection rate was therefore 1%. A limit, h = 2.5 ,was determined based on computer simulations (10,000 samples) to yield a false discovery rate of 9.9% and a true discovery rate of 75% over five years of monitoring.
References
1. Page ES. Continuous inspection schemes. Biometrika 1954;41: 100–115.
2. Marshall C, Best N, Bottle A, Aylin P. Statistical issues in the prospective monitoring of health outcomes across multiple units. J Roy Stat Soc A 2004;167: 541–559.
Rights and permissions
About this article
Cite this article
Biau, D.J., Leclerc, P., Marmor, S. et al. Monitoring the one year postoperative infection rate after primary total hip replacement. International Orthopaedics (SICOT) 36, 1155–1161 (2012). https://doi.org/10.1007/s00264-011-1444-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-011-1444-y