
Abstract
Objective
The objective was to retrospectively record the CT and MRI features and healing patterns of acute, incomplete stress fractures of the pars interarticularis.
Method
The CT scans of 156 adolescents referred with suspected pars interarticularis stress fractures were reviewed. Patients with incomplete (grade 2) pars fractures were included in the study. Fractures were assessed on CT according to vertebral level, location of cortical involvement and direction of fracture propagation. MRI was also performed in 72 of the 156 cases. MRI images of incomplete fractures were assessed for the presence of marrow oedema and cortical integrity. Fracture healing patterns were characterised on follow-up CT imaging.
Results
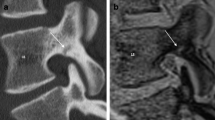
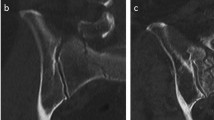
Twenty-five incomplete fractures were identified in 23 patients on CT. All fractures involved the inferior or infero-medial cortex of the pars and propagated superiorly or superolaterally. Ninety-two percent of incomplete fractures demonstrated either complete or partial healing on follow-up imaging. Two (8%) cases progressed to complete fractures. Thirteen incomplete fractures in 11 patients confirmed on CT also had MRI, and 92% demonstrated oedema in the pars. Ten out of thirteen fractures (77%) showed a break in the infero-medial cortex with intact supero-lateral cortex, which correlated with the CT findings. MRI incorrectly graded one case as a complete (grade 3) fracture, and 2 cases as (grade 1) stress reaction. Six fractures had follow-up MRI, 67% showed partial or complete cortical healing, and the same number showed persistent marrow oedema.
Conclusions
Incomplete fracture of the pars interarticularis represents a stage of the evolution of a complete stress fracture. The direction of fracture propagation is consistent, and complete healing can be achieved in most cases with appropriate clinical management. CT best demonstrates fracture size and extent, and is the most appropriate modality for follow-up. MRI is limited in its ability to fully depict the cortical integrity of incomplete fractures of the pars, but the presence of marrow oedema on fat-saturated T2-weighted sequences is a useful means of detecting acute spondylolysis.



Similar content being viewed by others

References
Ralston S, Weir M. Suspecting lumbar spondylolysis in adolescent low back pain. Clin Pediatr (Phila). 1998; 37(5): 287–293.
Fredrickson BE, Baker D, McHolick WJ, Yuan HA, Lubicky JP. The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am. 1984; 66(5): 699–707.
Coady CM, Micheli LJ. Stress fractures in the pediatric athlete. Clin Sports Med. 1997; 16(2): 225–238.
Kujala UM, Kinnunen J, Helenius P, Orava S, Taavitsainen M, Karaharju E. Prolonged low-back pain in young athletes: a prospective case series study of findings and prognosis. Eur Spine J. 1999; 8(6): 480–484.
Papanicolaou N, Wilkinson RH, Emans JB, Treves S, Micheli LJ. Bone scintigraphy and radiography in young athletes with low back pain. AJR Am J Roentgenol. 1985; 145: 1039–1044.
Pennell RG, Maurer AH, Bonakdarpour A. Stress injuries of the pars interarticularis: radiologic classification and indications for scintigraphy. AJR Am J Roentgenol. 1985; 145: 763–766.
Beutler WJ, Frederickson BE, Murtland A, Sweeney CA, Grant WD, Baker D. The natural history of spondylolysis and spondylolisthesis: 45-year follow-up evaluation. Spine. 2003; 28(10): 1027–1035; discussion 1035.
Saifuddin A, Burnett SJ. The value of lumbar spine MRI in the assessment of the pars interarticularis. Clin Radiol. 1997; 52(9): 666–671.
Hollenberg GM, Beattie PF, Meyers SP, Weinberg EP, Adams MJ. Stress reactions of the lumbar pars interarticularis: the development of a new MRI classification system. Spine. 2002; 27(2): 181–186.
Wiltse LL, Widell EH Jr, Jackson DW. Fatigue fracture: the basic lesion is isthmic spondylolisthesis. J Bone Joint Surg Am. 1975; 57(1): 17–22.
Johnson DW, Kessler JF, Ferrigni RG, Anderson JD. MR imaging of the pars interarticularis. AJR Am J Roentgenol. 1989; 152(2): 327–332.
Grenier N, Kressel HY, Schiebler ML, Grossman RI. Isthmic spondylolysis of the lumbar spine: MR imaging at 1.5 T. Radiology. 1989; 170(2): 489–493.
Ulmer JL, Elster AD, Mathews VP, Allen AM. Lumbar spondylolysis: reactive marrow changes seen in adjacent pedicles on MR images. AJR Am J Roentgenol. 1995; 164(2): 429–433.
Ulmer JL, Mathews VP, Elster AD, Mark LP, Daniels DL, Mueller W. MR imaging of lumbar spondylolysis: the importance of ancillary observations. AJR Am J Roentgenol. 1997; 169(1): 233–239.
Dutton JA, Hughes SP. SPECT in the management of patients with back pain and spondylolysis. Clin Nucl Med. 2000; 25(2): 93–96.
Gregory PL, Batt ME. SPECT and rg-CT findings in patients with back pain investigated for spondylolysis. Clin J Sport Med. 2005; 15(2): 79–86.
Campbell RSD, Grainger AJ, Hide IG, Papastefanou S, Greenough CG. Juvenile spondylolysis: comparative imaging of CT, SPECT and MRI. Skeletal Radiol. 2005; 34(2): 63–73.
Bland J, Bethem D, Moats W. Defects of pars interarticularis in athletes: a protocol for non-operative treatment. J Spinal Disord. 1993; 6(5): 406–411.
Miller SF, Congeni J, Swanson K. Long-term functional follow-up of early detected spondylolysis in young athletes. Am J Sports Med. 2004; 32(4): 928–933.
Herman MJ, Pizzutillo P. Spondylolysis and spondylolisthesis in the child and adolescent: a new classification. Clin Orthop Relat Res. 2005; 434: 46–54.
Grogan JP, Hemminghytt S, Williams AL, Carrera GF, Haughton VM. Spondylolysis with computed tomography. Radiology. 1982; 145: 737–742.
Langston JW, Gavant ML. “Incomplete Ring Sign”: a simple method for CT detection of spondylolysis. J Comput Assist Tomogr. 1985; 9: 726–729.
Mayor PE, Rees D. Spondylolysis, current imaging and management. Br J Radiol, published abstract, 2001.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dunn, A.J., Campbell, R.S.D., Mayor, P.E. et al. Radiological findings and healing patterns of incomplete stress fractures of the pars interarticularis. Skeletal Radiol 37, 443–450 (2008). https://doi.org/10.1007/s00256-008-0449-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-008-0449-0