
Abstract
Background
Pediatric patients requiring transfer to a dedicated children’s hospital from an outside institution may undergo CT imaging as part of their evaluation. Whether this imaging is performed prior to or after transfer has been shown to impact the radiation dose imparted to the patient. Other quality variables could also be affected by the pediatric experience and expertise of the scanning institution.
Objective
To identify differences in quality between abdominal CT scans and reports performed at a dedicated children’s hospital, and those performed at referring institutions.
Materials and methods
Fifty consecutive pediatric abdominal CT scans performed at outside institutions were matched (for age, gender and indication) with 50 CT scans performed at a dedicated freestanding children’s hospital. We analyzed the scans for technical parameters, report findings, correlation with final clinical diagnosis, and clinical utility. Technical evaluation included use of intravenous and oral contrast agents, anatomical coverage, number of scan phases and size-specific dose estimate (SSDE) for each scan. Outside institution scans were re-reported when the child was admitted to the children’s hospital; they were also re-interpreted for this study by children’s hospital radiologists who were provided with only the referral information given in the outside institution’s report. Anonymized original outside institutional reports and children’s hospital admission re-reports were analyzed by two emergency medicine physicians for ease of understanding, degree to which the clinical question was answered, and level of confidence in the report.
Results
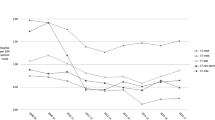
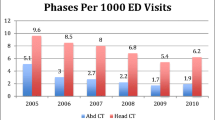
Mean SSDE was lower (8.68) for children’s hospital scans, as compared to outside institution scans (13.29, P = 0.03). Concordance with final clinical diagnosis was significantly lower for original outside institution reports (38/48, 79%) than for both the admission and study children’s hospital reports (48/50, 96%; P = 0.005). Children’s hospital admission reports were rated higher than outside institution reports for completeness, ease of understanding, answering of clinical question, and level of confidence of the report (P < 0.001).
Conclusion
Pediatric abdominal CT scans performed and interpreted at a dedicated children’s hospital are associated with higher technical quality, lower radiation dose and a more clinically useful report than those performed at referring institutions.
Similar content being viewed by others

References
Hartin CW Jr, Jordan JM, Gemme S et al (2013) Computed tomography scanning in pediatric trauma: opportunities for performance improvement and radiation safety. J Surg Res 180:226–231
Benedict LA, Paulus JK, Rideout L et al (2014) Are CT scans obtained at referring institutions justified prior to transfer to a pediatric trauma center? J Pediatr Surg 49:184–187
Nosek AE, Hartin CW Jr, Bass KD et al (2013) Are facilities following best practices of pediatric abdominal CT scans? J Surg Res 181:11–15
Sharp NE, Raghavan MU, Svetanoff WJ et al (2014) Radiation exposure — how do CT scans for appendicitis compare between a free standing children’s hospital and non-dedicated pediatric facilities? J Pediatr Surg 49:1016–1019
American College of Radiology (2014) Practice parameter for the performance of pediatric computed tomography (CT). http://www.acr.org/~/media/ACR/Documents/PGTS/guidelines/CT_Performing_Interpreting.pdf. Accessed 29 Oct 2016
American College of Radiology (1996) ACR appropriateness criteria: right lower quadrant pain — suspected appendicitis. https://acsearch.acr.org/docs/69357/Narrative/. Accessed 29 Oct 2016
American Association of Physicists in Medicine (2011) AAPM report no. 204: size-specific dose estimates (SSDE) in pediatric and adult body CT examinations. https://www.aapm.org/pubs/reports/RPT_204.pdf. Accessed 29 Oct 2016
Devers KJ, Brewster LR, Casalino LP (2003) Changes in hospital competitive strategy: a new medical arms race? Health Serv Res 38:447–469
Merenstein D, Egleston B, Diener-West M (2005) Lengths of stay and costs associated with children’s hospitals. Pediatrics 115:839–844
Ayanian JZ, Weissman JS (2002) Teaching hospitals and quality of care: a review of the literature. Milbank Q 80:569–593
Hopkins KL, Pettersson DR, Koudelka CW et al (2013) Size-appropriate radiation doses in pediatric body CT: a study of regional community adoption in the United States. Pediatr Radiol 43:1128–1135
Schappert SM, Bhuiya F (2006) Availability of pediatric services and equipment in emergency departments: United States, 2006. Natl Health Stat Rep 2012:1–21
Saito JM, Yan Y, Evashwick TW et al (2013) Use and accuracy of diagnostic imaging by hospital type in pediatric appendicitis. Pediatrics 131:e37–44
Eakins C, Ellis WD, Pruthi S et al (2012) Second opinion interpretations by specialty radiologists at a pediatric hospital: rate of disagreement and clinical implications. AJR Am J Roentgenol 199:916–920
Wieck MM, Hamilton NA, Krishnaswami S (2016) A cost and outcome analysis of pediatric single-incision appendectomy. J Surg Res 203:253–257
Acknowledgments
The authors gratefully acknowledge the assistance of Ms. Alison Clapp, library services manager at Boston Children’s Hospital. This research was supported by a 2013 Research Fellow grant to the lead author from the Society for Pediatric Radiology Research and Education Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Rights and permissions
About this article

Cite this article
Snow, A., Milliren, C.E., Graham, D.A. et al. Quality of pediatric abdominal CT scans performed at a dedicated children’s hospital and its referring institutions: a multifactorial evaluation. Pediatr Radiol 47, 391–397 (2017). https://doi.org/10.1007/s00247-016-3768-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-016-3768-7