
Abstract
Background
Complicated pleural effusion prolongs the hospital course of pneumonia. Chest tube placement with instillation of fibrinolytic medication allows efficient drain output and decreases hospital stay.
Objective
To evaluate experience with lower fibrinolytic dose for parapneumonic effusions and to assess potential dose stratification based on a simple ultrasound grading system.
Materials and methods
We retrospectively reviewed the medical record to identify children and young adults who received fibrinolytic therapy for parapneumonic effusion and had chest tube placement by an interventional radiology service at a single children’s hospital. We assessed tissue plasminogen activator (tPA) dosing and treatment duration, as well as the need for a second pleural procedure or surgical drainage. Diagnostic US images were classified as showing less than 50% pleural echogenicity (grade 1) or greater than 50% pleural echogenicity (grade 2) and were correlated with clinical parameters.
Results
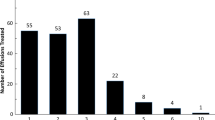
Of 32 patients with parapneumonic effusion, all except one received at least some 1-mg tPA doses. Dosing was solely 1-mg tPA in 81% of subjects; 19% of subjects also received 2-mg tPA doses. Mean fibrinolytic duration was 3.1 days for grade 1 effusions compared to 5.4 days for grade 2 effusions. A second pleural procedure was required in 15.6% of children. Pleural drainage with fibrinolytic therapy was successful in 97%; only one child required surgical drainage. Grade 2 US differed significantly from grade 1 US, with grade 2 occurring in younger patients (P < 0.0001), smaller patients (P < 0.0001), those needing a second procedure (P = 0.001), those with positive pleural culture or polymerase chain reaction test (P = 0.006), and those with longer treatment duration (P = 0.03).
Conclusion
A lower 1-mg dosing regimen of tissue plasminogen activator was effective in all children with less complex (grade 1 US imaging) parapneumonic effusions. Grade 2 US images correlated with younger and smaller children, presence of a pleural organism, and longer or more complicated chest tube duration.






Similar content being viewed by others

References
Balfour-Lynn IM, Abrahamson E, Cohen G et al (2005) BTS guidelines for the management of pleural infection in children. Thorax 60:i1–i21
Israel EN, Blackmer AB (2014) Tissue plasminogen activator for the treatment of parapneumonic effusions in pediatric patients. Pharmacotherapy 34:521–532
Cohen E, Mahant S, Dell SD et al (2012) The long-term outcomes of pediatric pleural empyema. Arch Pediatr Adolesc Med 166:999–1004
Feola GP, Shaw CA, Coburn L (2003) Management of complicated parapneumonic effusions in children. Tech Vasc Interv Radiol 6:197–204
Wells RG, Havens PL (2003) Intrapleural fibrinolysis for parapneumonic effusion and empyema in children. Radiology 228:370–378
Hawkins JA, Scaife ES, Hillman ND et al (2004) Current treatment of pediatric empyema. Semin Thorac Cardiovasc Surg 16:196–200
Gates RL, Hogan M, Weinstein S et al (2004) Drainage, fibrinolytics, or surgery: a comparison of treatment options in pediatric empyema. J Pediatr Surg 39:1638–1642
St. Peter SD, Tsao K, Spilde TL et al (2009) Thoracoscopic decortication vs. tube thoracostomy with fibrinolysis for empyema in children: a prospective, randomized trial. J Pediatr Surg 44:106–111
Weinstein M, Restrepo R, Chait PG et al (2004) Effectiveness and safety of tissue plasminogen activator in the management of complicated parapneumonic effusions. Pediatrics 113:e182–e185
Hogan MJ, Coley BD (2008) Interventional radiology treatment of empyema and lung abscesses. Paediatr Respir Rev 9:77–84
Ramnath RR, Heller RM, Ben-Ami T et al (1998) Implications of early sonographic evaluation of parapneumonic effusions in children with pneumonia. Pediatrics 101:68–71
Light RW (2011) Pleural controversy: optimal chest tube size for drainage. Respirology 16:244–248
Abu-Daff S, Maziak DE, Alshehab D et al (2013) Intrapleural fibrinolytic therapy (IPFT) in loculated pleural effusions — analysis of predictors for failure of therapy and bleeding: a cohort study. BMJ Open. doi:10.1136/bmjopen-2012-001887
Hendaus M, Abushahin A (2013) Intrapleural hemorrhage due to alteplase use in a 6-year-old boy with pleural effusion. Int J Gen Med 6:233–236
Finck C, Wagner C, Jackson R et al (2002) Empyema: development of a critical pathway. Semin Pediatr Surg 11:25–28
Park CS, Chung WM, Lim MK (1996) Transcatheter instillation of urokinase into loculated pleural effusion: analysis of treatment effect. AJR Am J Roentgenol 167:649–652
Kurian J, Levin TL, Han BK et al (2009) Comparison of ultrasound and CT in the evaluation of pneumonia complicated by parapneumonic effusion in children. AJR Am J Roentgenol 193:1648–1654
Acknowledgments
This project was supported by the Translational Research Institute (TRI) grant UL1TR000039 through the National Institutes of Health (NIH) National Center for Research Resources and National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not represent the official views of the NIH.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Rights and permissions
About this article

Cite this article
James, C.A., Braswell, L.E., Pezeshkmehr, A.H. et al. Stratifying fibrinolytic dosing in pediatric parapneumonic effusion based on ultrasound grade correlation. Pediatr Radiol 47, 89–95 (2017). https://doi.org/10.1007/s00247-016-3711-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-016-3711-y