
Abstract
Introduction
Currently, there is no reliable method to differentiate acute from chronic carotid occlusion. We propose a novel CTA-based method to differentiate acute from chronic carotid occlusions that could potentially aid clinical management of patients.
Methods
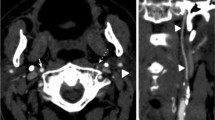
We examined 72 patients with 89 spontaneously occluded extracranial internal carotids with CT angiography (CTA). All occlusions were confirmed by another imaging modality and classified as acute (imaging <1 week of presumed occlusion) orchronic (imaging >4 weeks), based on circumstantial clinical and radiological evidence. A neuroradiologist and a neurologist blinded to clinical information determined the site of occlusion on axial sections of CTA. They also looked for (a) hypodensity in the carotid artery (thrombus), (b) contrast within the carotid wall (vasa vasorum), (c) the site of the occluded carotid, and (d) the “carotid ring sign” (defined as presence of a and/or b).
Results
Of 89 occluded carotids, 24 were excluded because of insufficient circumstantial evidence to determine timing of occlusion, 4 because of insufficient image quality, and 3 because of subacute timing of occlusion. Among the remaining 45 acute and 13 chronic occlusions, inter-rater agreement (kappa) for the site of proximal occlusion was 0.88, 0.45 for distal occlusion, 0.78 for luminal hypodensity, 0.82 for wall contrast, and 0.90 for carotid ring sign. The carotid ring sign had 88.9% sensitivity, 69.2% specificity, and 84.5% accuracy to diagnose acute occlusion.
Conclusion
The carotid ring sign helps to differentiate acute from chronic carotid occlusion. If further confirmed, this information may be helpful in studying ischemic symptoms and selecting treatment strategies in patients with carotid occlusions.






Similar content being viewed by others


References
Adams HP Jr, Bendixen BH, Leira E, Chang KC, Davis PH, Woolson RF, Clarke WR, Hansen MD (1999) Antithrombotic treatment of ischemic stroke among patients with occlusion or severe stenosis of the internal carotid artery: a report of the Trial of Org 10172 in Acute Stroke Treatment (TOAST). Neurology 53:122–125
De Silva DA, Brekenfeld C, Ebinger M, Christensen S, Barber PA, Butcher KS, Levi CR, Parsons MW, Bladin CF, Donnan GA, Davis SM (2010) The benefits of intravenous thrombolysis relate to the site of baseline arterial occlusion in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET). Stroke 41:295–299
Linfante I, Llinas RH, Selim M, Chaves C, Kumar S, Parker RA, Caplan LR, Schlaug G (2002) Clinical and vascular outcome in internal carotid artery versus middle cerebral artery occlusions after intravenous tissue plasminogen activator. Stroke 33:2066–2071
Rob CG (1969) Operation for acute completed stroke due to thrombosis of the internal carotid artery. Surgery 65:862–865
Mourand I, Brunel H, Vendrell JF, Thouvenot E, Bonafe A (2010) Endovascular stent-assisted thrombolysis in acute occlusive carotid artery dissection. Neuroradiology 52:135–140
Jovin TG, Gupta R, Uchino K, Jungreis CA, Wechsler LR, Hammer MD, Tayal A, Horowitz MB (2005) Emergent stenting of extracranial internal carotid artery occlusion in acute stroke has a high revascularization rate. Stroke 36:2426–2430
Aleksic M, Rueger MA, Lehnhardt FG, Sobesky J, Matoussevitch V, Neveling M, Heiss WD, Brunkwall J, Jacobs AH (2006) Primary stroke unit treatment followed by very early carotid endarterectomy for carotid artery stenosis after acute stroke. Cerebrovasc Dis 22:276–281
Flint AC, Duckwiler GR, Budzik RF, Liebeskind DS, Smith WS (2007) Mechanical thrombectomy of intracranial internal carotid occlusion: pooled results of the MERCI and Multi MERCI Part I trials. Stroke 38:1274–1280
Nedeltchev K, Brekenfeld C, Remonda L, Ozdoba C, Do DD, Arnold M, Mattle HP, Schroth G (2005) Internal carotid artery stent implantation in 25 patients with acute stroke: preliminary results. Radiology 237:1029–1037
Sugg RM, Malkoff MD, Noser EA, Shaltoni HM, Weir R, Cacayorin ED, Grotta JC (2005) Endovascular recanalization of internal carotid artery occlusion in acute ischemic stroke. AJNR Am J Neuroradiol 26:2591–2594
Michel P, Odier C, Rutgers M, Reichhart M, Maeder P, Meuli R, Wintermark M, Maghraoui A, Faouzi M, Croquelois A, Ntaios G (2010) The Acute Stroke Registry and Analysis of Lausanne (ASTRAL): design and baseline analysis of an ischemic stroke registry including acute multimodal imaging. Stroke 41:2491–2498
Watarai H, Kaku Y, Yamada M, Kokuzawa J, Tanaka T, Andoh T, Iwama T (2009) Follow-up study on in-stent thrombosis after carotid stenting using multidetector CT angiography. Neuroradiology 51:243–251
Chowdhury K, Bloom J, Black MJ, al-Noury K (1990) Spontaneous and nonspontaneous internal jugular vein thrombosis. Head Neck 12:168–173
Cohen JP, Persky MS, Reede DL (1985) Internal jugular vein thrombosis. Laryngoscope 95:1478–1482
Langer B, Kauffman P, Bechara M, Aguiar ET, Aun R (1991) Diagnosis of deep venous thrombosis of the lower limbs by computed tomography. Rev Paul Med 109:149–152
Menon BK, Singh J, Al-Khataami A, Demchuk AM, Goyal M (2010) The donut sign on CT angiography: an indicator of reversible intraluminal carotid thrombus? Neuroradiology 52:1055–1056
Conflict of interest
We declare that we have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Michel, P., Ntaios, G., Delgado, M.G. et al. CT angiography helps to differentiate acute from chronic carotid occlusion: the “carotid ring sign”. Neuroradiology 54, 139–146 (2012). https://doi.org/10.1007/s00234-011-0868-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00234-011-0868-9