
Abstract
Background
Paracetamol poisoning remains a leading cause of morbidity and mortality. Identifying indices of poor prognosis at first presentation is key to both improving clinical care and determining targets for intervention. Renal failure is a feature of severe paracetamol poisoning. The aim of this study was to investigate the relationship between renal function (serum creatinine, Cr) at first hospital presentation and time of tertiary referral to outcomes in severe paracetamol poisoning.
Methods
This was a retrospective cohort analysis of patients referred to the Scottish Liver Transplant Unit due to paracetamol poisoning between 1992 and 2004. The relation between degree of renal injury and outcomes, including worst prothrombin time, Kings College Hospital Criteria (KCHC) and death were examined. The effects of age, nature (single or multiple) and stated size of overdose, hepatic enzyme induction (gamma-glutamyl transpeptidase, GGT), degree of liver injury (aspartate aminotransferase, prothrombin time), blood pressure and renal injury were assessed.
Results
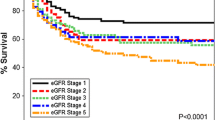
Data from 522 patients were included. Renal impairment (Cr >120 mmol/l) was present in 48.8% of patients with liver injury at time of first presentation. Creatinine at first admission predicted poorer outcome in terms of worse prothrombin time, KCHC and death (p < 0.001). Associated risk factors for renal dysfunction included later presentation, staggered ingestion, increased age, hypotension and elevated GGT at first admission.
Conclusions
Creatinine at first admission appears to be a predictor of poor outcome in paracetamol overdose. A better understanding of mechanisms involved in causing renal dysfunction may offer potential therapeutic targets for improving outcome in this common poisoning.

Similar content being viewed by others


References
Hawton K, Fagg J (1992) Trends in deliberate self poisoning and self injury in Oxford, 1976–90. Br Med J 304:1409–1411
Daley FFS, Fountain JS, Murray L, Graudins A, Buckley NA (2008) Guidelines for the management of paracetamol poisoning in Australia and New Zealand- explanation and elaboration. Med J Aust 188:296–301
Anonymous (2008) Poisoning. British National Formulary 55 (March 2008). RPS Publishing, London
Morgan OW, Griffiths C, Majeed A (2007) Interrupted time-series analysis of regulations to reduce paracetamol (acetaminophen) poisoning. PLoS Med 4:e105. doi:10.1371/journal.pmed.0040105
Bray GP (1993) Liver failure induced by paracetamol. Br Med J 306:157–158
Prescott LF (1983) Paracetamol overdosage. Pharmacological considerations and clinical management. Drugs 25:290–314
Boyer TD, Rouff SL (1971) Acetaminophen-induced hepatic necrosis and renal failure. JAMA 218:440–441
Curry RW Jr, Robinson JD, Sughrue MJ (1982) Acute renal failure after acetaminophen ingestion. JAMA 247:1012–1014
Kleinman JG, Breitenfield RV, Roth DA (1980) Acute renal failure associated with acetaminophen ingestion: report of a case and review of the literature. Clin Nephrol 14:201–205
Blakely P, McDonald BR (1995) Acute renal failure due to acetaminophen ingestion: a case report and review of the literature. J Am Soc Nephrol 6:48–53
Kher K, Makker S (1987) Acute renal failure due to acetaminophen ingestion without concurrent hepatotoxicity. Am J Med 82:1280–1281
O’Grady JG, Alexander GJ, Hayllar KM, Williams R (1989) Early indicators of prognosis in fulminant hepatic failure. Gastroenterology 97:439–445
Smilkstein MJ, Knapp GL, Kulig KW, Rumack BH (1988) Efficacy of oral N-acetylcysteine in the treatment of acetaminophen overdose. Analysis of the national multicenter study (1976 to 1985). N Engl J Med 319:1557–1562
Sivilotti ML, Yarema MC, Juurlink DN, Good AM, Johnson DW (2005) A risk quantification instrument for acute acetaminophen overdose patients treated with N-acetylcysteine. Ann Emerg Med 46:272–274
Jones AF, Harvey JM, Vale JA (1989) Hypophosphataemia and phosphaturia in paracetamol poisoning. Lancet 2:608–609
Mitchell JR, McMurtry RJ, Statham CN, Nelson SD (1977) Molecular basis for several drug-induced nephropathies. Am J Med 62:518–526
Trumper L, Girardi G, Elias MM (1992) Acetaminophen nephrotoxicity in male Wistar rats. Arch Toxicol 66:107–111
Pakravan N, Bateman DN, Goddard J (2007) Effect of acute paracetamol overdose on changes in serum and urine electrolytes. Br J Clin Pharmacol 64:824–832
von Mach MA, Hermanns-Clausen M, Koch I et al (2005) Experiences of a poison center network with renal insufficiency in acetaminophen overdose: an analysis of 17 cases. Clin Toxicol (Phila) 43:31–37
Boutis K, Shannon M (2001) Nephrotoxicity after acute severe acetaminophen poisoning in adolescents. J Toxicol Clin Toxicol 39:441–445
Beer C, Pakravan N, Hudson M et al (2007) Liver unit admission following paracetamol overdose with concentrations below current UK treatment thresholds. Q J Med 100:93–96
Mahadevan SB, McKiernan PJ, Davies P, Kelly DA (2006) Paracetamol induced hepatotoxicity. Arch Dis Child 91:598–603
Gorman DR, Bain M, Inglis JHC, Murphy D, Bateman DN (2007) How has legislation restricting paracetamol pack size affected patterns of deprivation related inequalities in self-harm in Scotland? Public Health 121:45–50
Acknowledgements
We gratefully acknowledge the assistance of Janice Davidson who maintains the database used for this study
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pakravan, N., Simpson, K.J., Waring, W.S. et al. Renal injury at first presentation as a predictor for poor outcome in severe paracetamol poisoning referred to a liver transplant unit. Eur J Clin Pharmacol 65, 163–168 (2009). https://doi.org/10.1007/s00228-008-0580-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-008-0580-9