
Abstract
Summary
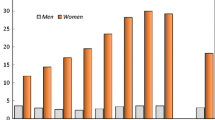
Age-specific and age-standardized associations between socioeconomic status (SES) and fractures in adults showed a social gradient of fracture, irrespective of fracture site. Compared to the highest SES, males in the lowest SES group had a sixfold increased odds for any fracture, whilst females had a twofold increased odds.
Introduction
The effective identification of predisposing risk factors for fracture requires understanding any association with SES. These investigations should consider both sexes, span the adult age range and include any fractures. We investigated age- and sex-specific and age-standardized associations between SES and fractures at any skeletal site in Australians aged ≥50 years.
Methods
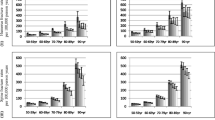
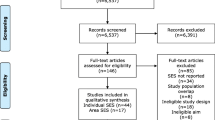
Incident fractures that occurred 2006–2007 for adults aged ≥50 years were identified from radiological reports extracted for the Barwon Statistical Division, in south-eastern Australia. SES was determined by cross-referencing residential addresses with Australian Bureau of Statistics census data and then categorized in quintiles. We compared frequencies of observed vs. expected fractures for SES quintiles using χ 2 comparison, calculated age-specific fracture incidence across SES and compared age-standardized fracture rates in SES quintile 1 to quintile 5.
Results
We identified 3943 incident fractures (69.4 % female); 47.4 % had occurred at major osteoporotic fracture (MOF) sites (hip, humerus, spine and forearm/wrist). Differences existed in observed vs. expected fractures across SES quintiles (p ≤ 0.001, sexes combined); all fractures showed an inverse association with SES (p ≤ 0.001, sexes combined). Compared to the highest SES quintile, individuals from the lowest SES quintile had between two to six times greater standardized fracture rates.
Conclusions
Disadvantaged men and women have an increased fracture incidence compared to their less disadvantaged counterparts. The large differences in fracture rates between SES groups warrant further research into designing appropriate, targeted interventions for those demographics at most risk.


Similar content being viewed by others
References
Johnell O, Kanis JA (2006) An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 17:1726
Watts J, Abimanyi-Ochom J, Sanders KM (2013) Osteoporosis costing all Australians: a new burden of disease analysis—2012 to 2022. In: Osteoporosis Australia, Glebe, NSW
Pasco JA, Sanders KM, Hoekstra FM, Henry MJ, Nicholson GC, Kotowicz MA (2005) The human cost of fracture. Osteoporos Int 16:2046–2052
Otmar R, Kotowicz MA, Brennan SL, Bucki-Smith G, Korn S, Pasco JA (2013) Personal and psychosocial impacts of clinical fracture in men. J Men’s Health 10:22–27
Center J, Nguyen TV, Schneider D et al (1999) Mortality after all major types of osteoporotic fracture in men and women: an observational study. Lancet 353:878
Holloway KL, Brennan SL, Kotowicz MA, Bucki-Smith G, Timney EN, Dobbins AG, Williams LJ, Pasco JA (2014) Prior fracture as a risk factor for future fracture in an Australian cohort. Osteoporos Int 9(1):196
Kanis JA, Johnell O, De Laet C et al (2004) A meta-analysis of previous fracture and subsequent fracture risk. Bone 35:375–382
Wilkinson RG, Pickett KE (2006) Income inequality and population health: a review and explanation of the evidence. Soc Sci Med 62:1768–1784
Wilkinson RG, Marmot MG (eds) (1998) Social determinants of health: the solid facts. WHO European Region, Copenhagen
WHO (2006) Commission on the Social Determinants of Health In Organisation GWH (ed) Fifth Meeting of the Commission on the Social Determinants of Health. Nairobi Kenya
Wilkinson R, Pickett K (2009) The spirit level: why more equal societies almost always do better. Allen Lane, London
Syddall HE, Evandrou M, Dennison EM, Cooper C, Sayer AA (2012) Social inequalities in osteoporosis and fracture among community-dwelling older men and women: findings from the Hertfordshire Cohort Study. Arch Osteoporos 7:37–48
Crandall CJ, Han W, Greendale GA, Seeman T, Tepper P, Thurston R, Karvonen-Gutierrez C, Karlamangla AS (2014) Socioeconomic status in relation to incident fracture risk in the Study of Women’s Health Across the Nation. Osteoporos Int 25:1379–1388
Brennan SL, Yan L, Lix LM, Morin SN, Majumdar SR, Leslie WD (2014) Sex and age-specific associations between income and incident major osteoporotic fractures in Canadian men and women: a population-based analysis. Osteoporos Int. doi:10.1007/s00198-00014-02914-z
Court-Brown CM, Aitken SA, Duckworth AD, Clement ND, McQueen MM (2013) The relationship between social deprivation and the incidence of adult fractures. J Bone Joint Surg Am 95:1–7
Brennan SL, Pasco JA, Urquhart DM, Oldenburg B, Hanna FS, Wluka AE (2009) The association between socioeconomic status and osteoporotic fracture in population-based adults: a systematic review. Osteoporos Int 49:165–171
Brennan SL, Henry MJ, Kotowicz MA, Nicholson GC, Zhang Y, Pasco JA (2011) Incident hip fracture and social disadvantage in an Australian population aged 50 years or greater. Bone 48:607–610
Pasco JA, Henry MJ, Gaudry TM, Nicholson GC, Kotowicz MA (1999) Identification of incident fractures: the Geelong Osteoporosis Study. Aust NZ J Med 29:203–206
ABS (2006) An introduction to socio-economic indexes for areas (SEIFA), 2006. In: ABS Cat No 20390
ABS (2006) Population by age and sex, regions of Australia, 2006, 3235.0. In: Australian Bureau of Statistics, Canberra
McNeill LH, Kreuter MW, Subramanian SV (2006) Social environment and physical activity: a review of concepts and evidence. Soc Sci Med 63
Gilman SE (2008) Educational attainment and cigarette smoking: a causal association? Int J Epidemiol 37:615–624
Lynch J, Kaplan G, Salonen J (1997) Why do poor people behave poorly? Variation in adult health behaviours and psychosocial characteristics by stages of the socioeconomic lifecourse. Soc Sci Med 44:809–819
Giesinger I, Goldblatt P, Howden-Chapman P, Marmot M, Kuh D, Brunner E (2013) Association of socioeconomic position with smoking and mortality: the contribution of early life circumstances in the 1946 birth cohort. J Epidemiol Community Health. doi:10.1136/jech-2013-203159
Kelsey JL, Prill MM, Keegan THM, Quesenberry CP, Sidney S (2005) Risk factors for pelvis fracture in older persons. Am J Epidemiol 162:879–886
Dunn JR (2000) Social inequality, population health, and housing: a study of two Vancouver neighborhoods. Soc Sci Med 51:563–587
Simpson A, Lamb S, Roberts PJ, Gardner TN, Grimley-Evans J (2004) Does the type of flooring affect the risk of hip fracture? Age Ageing 33:242–246
Stuck AE, Walthert JM, Nikolaus T, Bula CJ, Hohmann C, Beck JC (1999) Risk factors for functional status decline in community-living elderly people: a systematic review. Soc Sci Med 48:445–469
Beydoun MA, Popkin BM (2005) The impact of socio-economic factors on functional status decline among community-dwelling older adults in China. Soc Sci Med 60:2045–2057
Guimaraes RM (2007) Health capital, life course and ageing. Gerontology 53:96–101
Benzeval M, Judge K, Smaje C (1995) Beyond class, race and ethnicity: deprivation and health in Britain. Health Serv Res 30
(2009) U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, and the Centers for Medicare and Medicaid Services; U.S. Department of Health and Human Services; Centers for Disease Control and Prevention; Centers for Medicare and Medicaid Services. International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). Odum Institute V2.
Quah C, Boulton C, Moran C (2011) The influence of socioeconomic status on the incidence, outcome and mortality of fractures of the hip. J Bone Joint Surg Br 93-B:801–805
Turrell G, Stanley L, de Looper M, Oldenburg B (2006) Health inequalities in Australia: morbidity, health behaviours, risk factors and health service use. In: Canberra; Queensland University of Technology and the Australian Institute of Health and Welfare
Morgenstern H (1995) Ecologic studies in epidemiology: concepts, principles, and methods. Annu Rev Public Health 16:61–81
Acknowledgments
SLB was supported by a National Health and Medical Research Council (NHMRC) of Australia Early Career Fellowship (GNT1012472, 2011–2014) and an Alfred Deakin Postdoctoral Research Fellowship (2015–2016). LJW is supported by a NHMRC Career Development Fellowship (GNT1064272). The Geelong Osteoporosis Study Fracture Grid was developed with support from the Victorian Health Promotion Foundation and NHMRC (GNT 251638 and GNR 628582), the Geelong Region Medical Foundation and Amgen (Europe) GmBH.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Brennan, S.L., Holloway, K.L., Williams, L.J. et al. The social gradient of fractures at any skeletal site in men and women: data from the Geelong Osteoporosis Study Fracture Grid. Osteoporos Int 26, 1351–1359 (2015). https://doi.org/10.1007/s00198-014-3004-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-014-3004-y