
Abstract
Purpose
To measure and compare the amount of anterior tibial subluxation (ATS) after anatomic ACL reconstruction for both acute and chronic ACL-deficient patients.
Methods
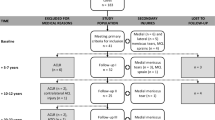
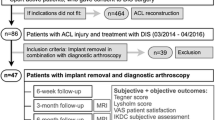
Fifty-two patients were clinically and radiographically evaluated after primary, unilateral, anatomic ACL reconstruction. Post-operative true lateral radiographs were obtained of both knees with the patient in supine position and knees in full passive extension with heels on a standardized bolster. ATS was measured on the radiographs by two independent and blinded observers. ATS was calculated as the side-to-side difference in tibial position relative to the femur. An independent t test was used to compare ATS between those undergoing anatomic reconstruction for an acute versus chronic ACL injury. Chronic ACL deficiency was defined as more than 12 weeks from injury to surgery.
Results
Patients averaged 26.4 ± 11.5 years (mean ± SD) of age, 43.6 % were female, and 48.1 % suffered an injury of the left knee. There were 30 and 22 patients in the acute and chronic groups, respectively. The median duration from injury to reconstruction for the acute group was 5 versus 31 weeks for the chronic group. After anatomic ACL reconstruction, the mean ATS was 1.0 ± 2.1 mm. There was no statistical difference in ATS between the acute and chronic groups (1.2 ± 2.0 vs. 0.6 ± 2.3 mm, n.s.). Assessment of inter-tester reliability for radiographic evaluation of ATS revealed an excellent intraclass correlation coefficient of 0.894.
Conclusions
Anatomic ACL reconstruction reduces ATS with a mean difference of 1.0 mm from the healthy contralateral limb. This study did not find a statistical difference in ATS between patients after anatomic ACL reconstruction in the acute or chronic phase. These observations suggest that anatomic ACL reconstruction, performed in either the acute or the chronic phase, approaches the normal AP relationship of the tibiofemoral joint.
Level of evidence
IV.


Similar content being viewed by others

References
Almekinders LC, de Castro D (2001) Fixed tibial subluxation after successful anterior cruciate ligament reconstruction. Am J Sports Med 29:280–283
Almekinders LC, Chiavetta JB (2001) Tibial subluxation in anterior cruciate ligament-deficient knees. Arthroscopy 17:960–962
Almekinders LC, Chiavetta JB, Clarke JP (1998) Radiographic evaluation of anterior cruciate ligament graft failure with special reference to tibial tunnel placement. Arthroscopy 14:206–211
Almekinders LC, Pandarinath R, Rahusen FT (2004) Knee stability following anterior cruciate ligament rupture and surgery. The contribution of irreducible tibial subluxation. J Bone Joint Surg Am 86-A:983–987
DeJour H, Walch G, Chambat P, Ranger P (1988) Active subluxation in extension. Am J Knee Surg 1:204–211
Forsythe B, Kopf S, Wong AK, Martins CAQ, Anderst W, Tashman S, Fu FH (2010) The location of femoral and tibial tunnels in anatomic double-bundle anterior cruciate ligament reconstruction analyzed by three-dimensional computed tomography models. J Bone Joint Surg Am 92:1418–1426
Franklin JL, Rosenberg TD, Paulos LE, France EP (1991) Radiographic assessment of instability of the knee due to rupture of the anterior cruciate ligament. A quadriceps-contraction technique. J Bone Joint Surg Am 73:365–372
Fukuta H, Takahashi S, Hasegawa Y, Ida K, Iwata H (2000) Passive terminal extension causes anterior tibial translation in some anterior cruciate ligament-deficient knees. J Orthop Sci 5:192–197
Ghodadra N, Mall NA, Karas V, Grumet RC, Kirk S, McNickle AG, Garrido CP, Cole BJ, Bach BR (2013) Articular and meniscal pathology associated with primary anterior cruciate ligament reconstruction. J Knee Surg 26(3):185–193
Hatayama K, Terauchi M, Saito K, Higuchi H, Yanagisawa S, Takagishi K (2013) The importance of tibial tunnel placement in anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy 29:1072–1078
Hussein M, van Eck CF, Cretnik A, Dinevski D, Fu FH (2012) Prospective randomized clinical evaluation of conventional single-bundle, anatomic single-bundle, and anatomic double-bundle anterior cruciate ligament reconstruction: 281 cases with 3- to 5-year follow-up. Am J Sports Med 40:512–520
Iriuchishima T, Shirakura K, Fu FH (2013) Graft impingement in anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 21(3):664–670
Magnussen RA, Pedroza AD, Donaldson CT, Flanigan DC, Kaeding CC (2013) Time from ACL injury to reconstruction and the prevalence of additional intra-articular pathology: is patient age an important factor? Knee Surg Sports Traumatol Arthrosc 21(9):2029–2034
Mishima S, Takahashi S, Kondo S, Ishiguro N (2005) Anterior tibial subluxation in anterior cruciate ligament-deficient knees: quantification using magnetic resonance imaging. Arthroscopy 21:1193–1196
Tanaka MJ, Jones KJ, Gargiulo AM, Delos D, Wickiewicz TL, Potter HG, Pearle AD (2013) Passive anterior tibial subluxation in anterior cruciate ligament-deficient knees. Am J Sports Med 41:2347–2352
Tashman S, Collon D, Anderson K, Kolowich P, Anderst W (2004) Abnormal rotational knee motion during running after anterior cruciate ligament reconstruction. Am J Sports Med 32:975–983
Vahey TN, Hunt JE, Shelbourne KD (1993) Anterior translocation of the tibia at MR imaging: a secondary sign of anterior cruciate ligament tear. Radiology 187:817–819
Van Eck CF, Lesniak BP, Schreiber VM, Fu FH (2010) Anatomic single- and double-bundle anterior cruciate ligament reconstruction flowchart. Arthroscopy 26:258–268
Zuiderbaan HA, Khamaisy S, Nawabi DH, Thein R, Nguyen JT, Lipman JD, Pearle AD (2014) Notchplasty in anterior cruciate ligament reconstruction in the setting of passive anterior tibial subluxation. Knee 21:1160–1165
Acknowledgments
The authors thank the Radiology Section, Center for Sports Medicine, University of Pittsburgh Medical Center, for their help and cooperation in this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Muller, B., Duerr, E.R.H., van Dijk, C.N. et al. Anatomic anterior cruciate ligament reconstruction: reducing anterior tibial subluxation. Knee Surg Sports Traumatol Arthrosc 24, 3005–3010 (2016). https://doi.org/10.1007/s00167-015-3612-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3612-x