
Abstract
Purpose
Among patients surviving treatment in intensive care units (ICU), some cases exist for which inflammation persisted with prolonged hospital stays, referred as persistent inflammatory, immunosuppressed, catabolic syndrome (PIICS). C reactive protein (CRP) is regarded as the most important marker for PIICS. Nevertheless, the applicable cut-off of CRP for PIICS has never been described in the literature.
Methods
Data of patients admitted to the ICU/Emergency ward from May 2015 through June 2019 were analyzed retrospectively. Using K-means clustering, a 14-day CRP transition dataset was analyzed and categorized finally into 7 classes: 4 PIICS classes and 3 non-PIICS classes. Outcomes and the other PIICS characteristics were evaluated.
Results
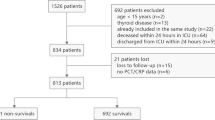
From all 5513 admitted patients, this study examined data of 539 patients who had been admitted for more than 14 days, and for whom 14 day CRP transition analysis could be performed. By the CRP transitions of 7 categorized classes, the CRP cut-off for PIICS was regarded as 3.0 mg/dl on day 14. The Barthel Index at discharge, albumin, and total lymphocyte counts on day 14 were significantly lower in PIICS classes than those of non-PIICS classes. Creatinine kinase, antithrombin activity and thrombomodulin on admission were regarded as independent risk factors for PIICS.
Conclusions
Among patients with prolonged hospital stay, the PIICS population had elevated CRP, but lower Barthel Index, albumin, and total lymphocyte counts. The criterion of day 14 CRP for PIICS should be 3.0 mg/dl.


Similar content being viewed by others

References
Needham DM, Davidson J, Cohen H et al (2012) Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med 40(2):502–509
Elliott D, Davidson JE, Harvey MA et al (2014) Exploring the scope of post-intensive care syndrome therapy and care: engagement of non-critical care providers and survivors in a second stakeholders meeting. Crit Care Med 42(12):2518–2526
Kahn JM, Le T, Angus DC et al (2015) The epidemiology of chronic critical illness in the United States. Crit Care Med 43(2):282–287
Stortz JA, Mira JC, Raymond SL et al (2018) Benchmarking clinical outcomes and the immunocatabolic phenotype of chronic critical illness after sepsis in surgical intensive care unit patients. J Trauma Acute Care Surg 84(2):342–349
Rosenthal MD, Moore FA (2015) Persistent inflammatory, immunosuppressed, catabolic syndrome (PICS): a new phenotype of multiple organ failure. J Adv Nutr Hum Metab 1(1):e784
Gentile LF, Cuenca AG, Efron PA et al (2012) Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care. J Trauma Acute Care Surg 72(6):1491–1501
Mira JC, Gentile LF, Mathias BJ et al (2017) Sepsis pathophysiology, chronic critical illness, and persistent inflammation-immunosuppression and catabolism syndrome. Crit Care Med 45(2):253–262
Hawkins RB, Raymond SL, Stortz JA et al (2018) Chronic critical illness and the persistent inflammation, immunosuppression, and catabolism syndrome. Front Immunol 9:1511
Yang N, Li B, Ye B et al (2017) The long-term quality of life in patients with persistent inflammation-immunosuppression and catabolism syndrome after severe acute pancreatitis: a retrospective cohort study. J Crit Care 42:101–106
Pedregosa F, Varoquaux G, Gramfort A et al (2011) Scikit-learn: machine learning in python. J Machine Learn Res 12:6
Lloyd SP (1982) Least squares quantization in PCM. IEEE Trans Inform Theory 28:129–137
Gabay C, Kushner I (1999) Acute-phase proteins and other systemic responses to inflammation. N Engl J Med 340(6):448–454
Gauldie J, Richards C, Harnish D, Lansdorp P, Baumann H (1987) Interferon beta 2/B-cell stimulatory factor type 2 shares identity with monocyte-derived hepatocyte-stimulating factor and regulates the major acute phase protein response in liver cells. Proc Natl Acad Sci USA 84(20):7251–7255
Morris-Stiff G, Gomez D, Prasad KR (2008) C-reactive protein in liver cancer surgery. Eur J Surg Oncol 34(7):727–729
Le Gall C, Désidéri-Vaillant C, Nicolas X (2011) Significations of extremely elevated C-reactive protein: about 91 cases in a French hospital center. Pathol Biol (Paris) 59(6):319–320
Wu JY, Lee SH, Shen CJ et al (2012) Use of serum procalcitonin to detect bacterial infection in patients with autoimmune diseases: a systematic review and meta-analysis. Arthritis Rheum 64(9):3034–3042
Woloshin S, Schwartz LM (2005) Distribution of C-reactive protein values in the United States. N Engl J Med 352(15):1611–1613
Kushner I, Antonelli MJ (2015) What should we regard as an “elevated” C-reactive protein level? Ann Intern Med 163(4):326
Black S, Kushner I, Samols D (2004) C-reactive Protein. J Biol Chem 279(47):48487–48490
Marnell L, Mold C, Du Clos TW (2005) C-reactive protein: ligands, receptors and role in inflammation. Clin Immunol 117(2):104–111
Volanakis JE (2001) Human C-reactive protein: expression, structure, and function. Mol Immunol 38(2–3):189–197
Griselli M, Herbert J, Hutchinson WL et al (1999) C-reactive protein and complement are important mediators of tissue damage in acute myocardial infarction. J Exp Med 190(12):1733–1740
Moshage HJ, Janssen JA, Franssen JH, Hafkenscheid JC, Yap SH (1987) Study of the molecular mechanism of decreased liver synthesis of albumin in inflammation. J Clin Invest 79(6):1635–1641
Moldawer LL, Copeland EM (1997) Proinflammatory cytokines, nutritional support, and the cachexia syndrome: interactions and therapeutic options. Cancer 79(9):1828–1839
Schefold JC, Bierbrauer J, Weber-Carstens S (2010) Intensive care unit-acquired weakness (ICUAW) and muscle wasting in critically ill patients with severe sepsis and septic shock. J Cachexia Sarcopenia Muscle 1(2):147–157
Callahan LA, Supinski GS (2009) Sepsis-induced myopathy. Crit Care Med 37(10 Suppl):S354–S367
Foley JH, Conway EM (2016) Cross talk pathways between coagulation and inflammation. Circ Res 118(9):1392–1408
Conway EM (2012) Thrombomodulin and its role in inflammation. Semin Immunopathol 34(1):107–125
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors state that they have no conflict of interest. Kentaro Ogura and Tomohiro Sonoo are employed by TXP Medical Co. Ltd.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nakamura, K., Ogura, K., Nakano, H. et al. C-reactive protein clustering to clarify persistent inflammation, immunosuppression and catabolism syndrome. Intensive Care Med 46, 437–443 (2020). https://doi.org/10.1007/s00134-019-05851-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-019-05851-3