
Avoid common mistakes on your manuscript.
Acute respiratory distress syndrome (ARDS) was first described 1967 [1]. Mortality is high, around 30–40 %, with only slow decrease over the years. How can one then say that there are physiologic advances that have improved pulmonary treatment? One reason is that patients with increasing disease severity and increasing age are more frequently admitted to intensive care units and there receive the diagnosis of ARDS. Earlier they may have been lost before any diagnosis was made.
Below are listed ten physiologic advances that have been of importance to understand the pathophysiology of ARDS and have guided improvements in treatment.
-
1.
Imaging pulmonary pathophysiology
Imaging methods such as computerized tomography, electrical impedance tomography, positron emission tomography, and ultrasound have helped us to understand the pathophysiology of ARDS [2]. Imaging techniques have also enabled regional analysis of lung function and distribution of inflammation, the latter providing new information on ventilator-induced lung injury (VILI). These advances have guided new treatment and “fine-tuning” of existing treatment, in particular in optimizing ventilator support. Figure 1 shows examples of visualization of morphological abnormalities, of lung function, and of sites of inflammation in the lung.
Fig. 1 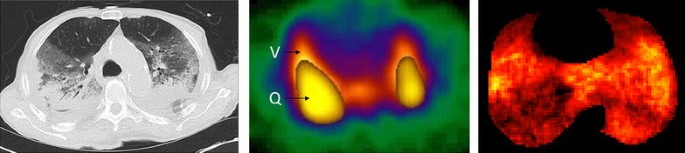
Axial images of lung morphology assessed by computed tomography (CT; left panel), lung function (ventilation and perfusion) by single photon emission computed tomography (SPECT; middle panel), and lung inflammation by positron emission tomography (PET; right panel) in clinical (CT) and experimental (SPECT, PET) ARDS. Left panel CT image with pulmonary window displaying bilateral dorsal consolidations with air bronchogram. Further anterior is a layer of ground glass opacities and most anterior is normal-appearing lung parenchyma. By courtesy of Tomas Hansen, Department of Radiology, University Hospital, Uppsala, Sweden. Middle panel Distributions of ventilation (V) and perfusion (Q) obtained by inhalation of short-lived krypton gas (81mKr) and intravenous injection of microspheres labelled with technetium (99mTc). Note ventilation in anterior regions without perfusion and perfusion in dependent regions without ventilation. By courtesy of Enn Maripuu, Department of Hospital Physics, University hospital, Uppsala, Sweden. Right panel Distribution of inflammation obtained by intravenous injection of radioactive 18F-fluorodeoxyglucose. Note predominance of inflammation in the mid regions of the lung, sparing the anterior and also most of the dorsal regions. By courtesy of Joao Batista Borges, Department of Surgical Sciences, Uppsala University, Uppsala, Sweden
-
2..
Baby lung and protective ventilation
A large part of the ARDS lung is initially collapsed or poorly aerated or overinflated. Ventilated lung volume is dramatically reduced. This lung is nicknamed “baby lung” because only one-third or one-fourth of a normal lung is available for ventilation [3]. Harmful stretches driven to the ventilated “baby lung” with ventilation set to “normal lungs” have been demonstrated, initiating not only baro/volutrauma but also biotrauma. Strategies to minimize collapse and overdistension have been emphasized in order to create “protective ventilation”. Tidal volume (V T) has been reduced from 12 to 15 ml/kg body weight (once assumed to facilitate gas exchange) to 6 ml/kg predicted body weight (the predicted weight being a better way to adapt to lung size) [4] with further possible decrease. This simple approach is life-saving.
-
3.
Driving pressure
Decreasing V T or increasing end-expiratory lung volume both reduce the lung stretch that is frequently expressed as stress (external forces) and strain (internal deformation). Driving pressure (DP), i.e., the difference between end-inspiratory and end-expiratory airway pressure, can be considered a clinical estimate of stress (pressure) and strain (relation to lung volume) as it is inversely proportional to respiratory compliance [5]. It contains information that reflects both disease severity and the effects of V T and pressure settings. Ventilator settings and lung conditions that enable lower DP result in better survival.
-
4.
Lung recruitment and PEEP titration
Reopening collapsed lung reduces shunt and possibly strain. An open lung should be less prone to inflammation and less strain should decrease VILI. Once recruited, the lung should stay open and this can be achieved by titrating an optimum PEEP. How to perform the recruitment maneuver and how to select patients recruitable with high PEEP are still under debate [6, 7]. Whether this requires the systematic recording of transpulmonary pressure is another issue that causes debate.
-
5.
Prone position
Prone position may improve outcome in severe ARDS [8]. It seems to create a more homogeneous distribution of ventilation, perfusion, and possibly reduced lung strain. The last of these can be expected if ventilation is distributed in proportion to regional lung volume. It may be that improved outcome by using prone position is not necessarily related to improved gas exchange but rather to decrease in regional lung strain.
-
6.
Avoiding intubation
The pathophysiology of acute respiratory failure at an early stage is a complex interplay between a high level of work of breathing [9] and blood flow redistribution towards the respiratory muscles while there are theoretical concerns that the high levels of ventilation may lead to lung injury. Interestingly, high flow nasal cannula therapy seems to offer the best approach to minimize the risks associated with intubation and mechanical ventilation and improve survival [10].
-
7.
Managing spontaneous breathing
The recent observations concerning patient–ventilator asynchrony and its association with mortality [11] explain in part that the management of spontaneous breathing remains so complex and why, at the initial stage, a complete paralysis of the respiratory muscles may help to decrease strain and improve survival [12]. Several mechanisms may be at play, causing a deleterious interaction of spontaneous and mechanical breathing (such as local increases in strain, reflex contractions occurring under deep sedation [13] as well as breath stacking). There is a need for a closer monitoring which, as a result, may allow titrating respiratory muscle activity. Preserving respiratory muscle function also has a lot of potential benefits and seems essential at the weaning stage [14].
-
8.
Shifting our objectives for gas exchange
For many years higher oxygenation and normalized alveolar ventilation were the objectives of mechanical ventilation. Pioneer works in ARDS showed that the price to pay for “normalizing” these physiologic variables was lung injury. This major conceptual shift allowed us to accept trade-offs, with thresholds still under investigations, especially regarding PaCO2 levels. We also completely shifted the early concept of the “ventilator lung” being caused by high FIO2 to being caused by excessive strain [15]. As often occurs in medicine, we may rediscover in the future that oxygen toxicity does play some role.
-
9.
Understanding the determinants of oxygenation
Because oxygenation is still the number one parameter observed by clinicians, understanding its determinants in the context of ARDS has enormously helped the individualization of ventilatory and hemodynamic management. Indeed, oxygenation is influenced by alveolar recruitment, but also by venous blood saturation and shunt (both influenced by cardiac output), FIO2, and intracardiac shunt [16]. The complex nature of these relationships means that an optimal management needs a good understanding of physiology.
-
10.
Understanding when ventilation is not enough
Acknowledging that mechanical ventilation is causing excessive strain has led to the concept of completely or partially resting the lung, early in the history of ARDS. Complete lung rest is obtained with extracorporeal membrane oxygenation and seems to be reserved for severe cases, while partial rest obtained with CO2 removal techniques offers an exciting alternative to our current standards [17].

Conclusion: bedside pathophysiology is the key for translational research
Progress in ARDS research has been driven by epidemiology, experimental research, and bedside physiology. Ignoring one of these three components (or thinking that one of them will solve everything) leads to wasting time, energy, and money at the expense of patients. The key for future translational research, hopefully integrating biologic markers for diagnosis and classification, will continue to need a better understanding of mechanisms.
References
Ashbaugh DG, Bigelow DB, Petty TL, Levine BE (1967) Acute respiratory distress in adults. Lancet 2:319–323
Bellani G, Mauri T, Pesenti A (2012) Imaging in acute lung injury and acute respiratory distress syndrome. Curr Opin Crit Care 18:29–34
Gattinoni L, Marini JJ, Pesenti A, Quintel M, Mancebo J, Brochard L (2016) The “baby lung” became an adult. Intensive Care Med. doi:10.1007/s00134-015-4200-8
The Acute Respiratory Distress Syndrome Network (2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 342:1301–1308 (2000)
Amato MB, Meade MO, Slutsky AS, Brochard L, Costa EL, Schoenfeld DA, Stewart TE, Briel M, Talmor D, Mercat A, Richard JC, Carvalho CR, Brower RG (2015) Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med 372:747–755
Keenan JC, Formenti P, Marini JJ (2014) Lung recruitment in acute respiratory distress syndrome: what is the best strategy? Curr Opin Crit Care 20:63–68
Goligher EC, Kavanagh BP, Rubenfeld GD, Adhikari NK, Pinto R, Fan E, Brochard LJ, Granton JT, Mercat A, Marie Richard JC, Chretien JM, Jones GL, Cook DJ, Stewart TE, Slutsky AS, Meade MO, Ferguson ND (2014) Oxygenation response to positive end-expiratory pressure predicts mortality in acute respiratory distress syndrome. A secondary analysis of the LOVS and ExPress trials. Am J Respir Crit Care Med 190(1):70–76
Guerin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, Mercier E, Badet M, Mercat A, Baudin O, Clavel M, Chatellier D, Jaber S, Rosselli S, Mancebo J, Sirodot M, Hilbert G, Bengler C, Richecoeur J, Gainnier M, Bayle F, Bourdin G, Leray V, Girard R, Baboi L, Ayzac L, PROSEVA Study Group (2013) Prone positioning in severe acute respiratory distress syndrome. N Engl J Med 368:2159–2168
L’Her E, Deye N, Lellouche F, Taille S, Demoule A, Fraticelli A, Mancebo J, Brochard L (2005) Physiologic effects of noninvasive ventilation during acute lung injury. Am J Respir Crit Care Med 172:1112–1118
Frat JP, Thille AW, Mercat A, Girault C, Ragot S, Perbet S, Prat G, Boulain T, Morawiec E, Cottereau A, Devaquet J, Nseir S, Razazi K, Mira JP, Argaud L, Chakarian JC, Ricard JD, Wittebole X, Chevalier S, Herbland A, Fartoukh M, Constantin JM, Tonnelier JM, Pierrot M, Mathonnet A, Beduneau G, Deletage-Metreau C, Richard JC, Brochard L, Robert R, FLORALI Study Group, REVA Network (2015) High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med 372:2185–2196
Blanch L, Villagra A, Sales B, Montanya J, Lucangelo U, Lujan M, Garcia-Esquirol O, Chacon E, Estruga A, Oliva JC, Hernandez-Abadia A, Albaiceta GM, Fernandez-Mondejar E, Fernandez R, Lopez-Aguilar J, Villar J, Murias G, Kacmarek RM (2015) Asynchronies during mechanical ventilation are associated with mortality. Intensive Care Med 41:633–641
Papazian L, Forel JM, Gacouin A, Penot-Ragon C, Perrin G, Loundou A, Jaber S, Arnal JM, Perez D, Seghboyan JM, Constantin JM, Courant P, Lefrant JY, Guerin C, Prat G, Morange S, Roch A (2010) Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med 363:1107–1116
Akoumianaki E, Lyazidi A, Rey N, Matamis D, Perez-Martinez N, Giraud R, Mancebo J, Brochard L, Marie Richard JC (2013) Mechanical ventilation-induced reverse-triggered breaths: a frequently unrecognized form of neuromechanical coupling. Chest 143:927–938
Goligher EC, Fan E, Herridge MS, Murray A, Vorona S, Brace D, Rittayamai N, Lanys A, Tomlinson G, Singh JM, Bolz SS, Rubenfeld GD, Kavanagh BP, Brochard LJ, Ferguson ND (2015) Evolution of diaphragm thickness during mechanical ventilation. Impact of inspiratory effort. Am J Respir Crit Care Med 192:1080–1088
Dreyfuss D, Saumon G (1998) Ventilator-induced lung injury: lessons from experimental studies. Am J Respir Crit Care Med 157:294–323
Mekontso Dessap A, Boissier F, Leon R, Carreira S, Campo FR, Lemaire F, Brochard L (2010) Prevalence and prognosis of shunting across patent foramen ovale during acute respiratory distress syndrome. Crit Care Med 38:1786–1792
Gattinoni L, Carlesso E, Langer T (2012) Towards ultraprotective mechanical ventilation. Curr Opin Anaesthesiol 25:141–147
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Brochard, L., Hedenstierna, G. Ten physiologic advances that improved treatment for ARDS. Intensive Care Med 42, 814–816 (2016). https://doi.org/10.1007/s00134-016-4320-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-016-4320-9