
Abstract
Objective
To determine whether hyperglycemia exerts deleterious effects via cerebral energy metabolism and to illuminate the effects of cerebral high/low glucose in patients with aneurysmal subarachnoid hemorrhage.
Design and setting
Prospective, nonrandomized single-center study over a 2-year period in an intensive care unit at a primary-level university hospital.
Patients
28 subarachnoid hemorrhage patients (age 53 ± 10 years, WFNS grade 2.8 ± 1.5) classified as asymptomatic (n = 5) or symptomatic with acute focal or delayed ischemic neurological deficits (n = 23).
Measurements and results
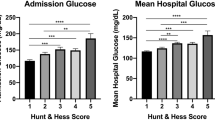
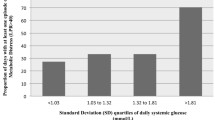
Hyperglycemia (> 7.8 mmol/l; > 140 mg/dl) was more frequent in symptomatic patients and was reflected in higher glycerol concentrations than in asymptomatic patients. In all patients a microdialysis catheter was inserted into the tissue at risk; dialysates were collected hourly for 10 days. Cerebral low-glucose episodes (< 0.6 mmol/l) and high-glucose episodes (> 2.6 mmol/l) occurred independently of blood glucose levels. During high-glucose episodes cerebral microdialysate levels were normal, while cerebral low glucose, occurring more frequently in symptomatic patients, was associated with severe cellular distress (increase in lactate/pyruvate ratio, glutamate, glycerol) and with unfavorable outcome if combined with hyperglycemia.
Conclusions
Although hyperglycemia was more frequent in symptomatic patients and associated with high glycerol levels, hyperglycemia was not related to cerebral high glucose. It appears that the association of adverse outcome with acute-phase hyperglycemia is not mediated by cerebral glucose metabolism. Cerebral low glucose was associated with severe metabolic distress and may present a target for therapy to improve clinical outcome.




Similar content being viewed by others

References
Lanzino G, Kassell NF, Germanson T, Truskowski L, Alves W (1993) Plasma glucose levels and outcome after aneurysmal subarachnoid hemorrhage. J Neurosurg 79:885–891
Alberti O, Becker R, Benes L, Wallenfang T, Bertalanffy H (2000) Initial hyperglycemia as an indicator of severity of the ictus in poor-grade patients with spontaneous subarachnoid hemorrhage. Clin Neurol Neurosurg 102:78–83
Frontera JA, Fernandez A, Claassen J, Schmidt M, Schumacher HC, Wartenberg K, Temes R, Parra A, Ostapkovich ND, Mayer SA (2006) Hyperglycemia after SAH: predictors, associated complications, and impact on outcome. Stroke 37:199–203
Seaquist ER, Damberg GS, Tkac I, Gruetter R (2001) The effect of insulin on in vivo cerebral glucose concentrations and rates of glucose transport/metabolism in humans. Diabetes 50:2203–2209
Bell DA, Strong AJ (2005) Glucose/insulin infusions in the treatment of subarachnoid haemorrhage: a feasibility study. Br J Neurosurg 19:21–24
Hlatky R, Valadka AB, Goodman JC, Contant CF, Robertson CS (2004) Patterns of energy substrates during ischemia measured in the brain by microdialysis. J Neurotrauma 21:894–906
Unterberg AW, Sakowitz OW, Sarrafzadeh AS, Benndorf G, Lanksch WR (2001) Role of bedside microdialysis in the diagnosis of cerebral vasospasm following aneurysmal subarachnoid hemorrhage. J Neurosurg 94:740–749
Hutchinson PJ, Gupta AK, Fryer TF, Al-Rawi PG, Chatfield DA, Coles JP, O'Connell MT, Kett-White R, Minhas PS, Aigbirhio FI, Clark JC, Kirkpatrick PJ, Menon DK, Pickard JD (2002) Correlation between cerebral blood flow, substrate delivery, and metabolism in head injury: a combined microdialysis and triple oxygen positron emission tomography study. J Cereb Blood Flow Metab 22:735–745
Ungerstedt U (1991) Microdialysis-principles and applications for studies in animals and man. J Intern Med 230:365–373
Kerner A, Schlenk F, Sakowitz O, Haux D, Sarrafzadeh A (2007) Impact of hyperglycemia on neurological deficits and extracellular glucose levels in aneurysmal subarachnoid hemorrhage patients. Neurol Res 29:647–653
Fisher CM, Kistler JP, Davis JM (1980) Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning. Neurosurgery 6:1–9
Drake C (1988) Report of World Federation of Neurological Surgeons Committee on a Universal Subarachnoid Hemorrhage Grading Scale. J Neurosurg 68:985–986
Lanzino G, Kassell NF (1999) Double-blind, randomized, vehicle-controlled study of high-dose tirilazad mesylate in women with aneurysmal subarachnoid hemorrhage. II. A cooperative study in North America. J Neurosurg 90:1018–1024
Jennett B, Bond M (1975) Assessment of outcome after severe brain damage. Lancet I:480–484
Reinstrup P, Stahl N, Mellergard P, Uski T, Ungerstedt U, Nordstrom CH (2000) Intracerebral microdialysis in clinical practice: baseline values for chemical markers during wakefulness, anesthesia, and neurosurgery. Neurosurgery 47:701–709
Hutchinson PJ, O'Connell MT, Al-Rawi PG, Maskell LB, Kett-White R, Gupta AK, Richards HK, Hutchinson DB, Kirkpatrick PJ, Pickard JD (2000) Clinical cerebral microdialysis: a methodological study. J Neurosurg 93:37–43
Vespa P, Bergsneider M, Hattori N, Wu HM, Huang SC, Martin NA, Glenn TC, McArthur DL, Hovda DA (2005) Metabolic crisis without brain ischemia is common after traumatic brain injury: a combined microdialysis and positron emission tomography study. J Cereb Blood Flow Metab 25:763–774
Sarrafzadeh A, Haux D, Kuchler I, Lanksch WR, Unterberg AW (2004) Poor-grade aneurysmal subarachnoid hemorrhage: relationship of cerebral metabolism to outcome. J Neurosurg 100:400–406
Sarrafzadeh AS, Sakowitz OW, Kiening KL, Benndorf G, Lanksch WR, Unterberg AW (2002) Bedside microdialysis: a tool to monitor cerebral metabolism in subarachnoid hemorrhage patients? Crit Care Med 30:1062–1070
Robertson CS, Clifton GL, Grossman RG, Ou CN, Goodman JC, Borum P, Bejot S, Barrodale P (1988) Alterations in cerebral availability of metabolic substrates after severe head injury. J Trauma 28:1523–1532
Wass CT, Lanier WL (1996) Glucose modulation of ischemic brain injury: review and clinical recommendations. Mayo Clin Proc 71:801–812
Badjatia N, Topcuoglu MA, Buonanno FS, Smith EE, Nogueira RG, Rordorf GA, Carter BS, Ogilvy CS, Singhal AB (2005) Relationship between hyperglycemia and symptomatic vasospasm after subarachnoid hemorrhage. Crit Care Med 33:1603–1609
Van den Berghe G, Schoonheydt K, Becx P, Bruyninckx F, Wouters PJ (2005) Insulin therapy protects the central and peripheral nervous system of intensive care patients. Neurology 64:1348–1353
Berek K, Kiechl S, Pfausler B, Auckenthaler A, Schmutzhard E (1992) Prognostic indices in subarachnoid haemorrhage. Lancet 339:68
Woo E, Ma JT, Robinson JD, Yu YL (1988) Hyperglycemia is a stress response in acute stroke. Stroke 19:1359–1364
Schurr A, Payne RS, Miller JJ, Tseng MT (2001) Preischemic hyperglycemia-aggravated damage: evidence that lactate utilization is beneficial and glucose-induced corticosterone release is detrimental. J Neurosci Res 66:782–789
Berger L, Hakim AM (1986) The association of hyperglycemia with cerebral edema in stroke. Stroke 17:865–871
Song EC, Chu K, Jeong SW, Jung KH, Kim SH, Kim M, Yoon BW (2003) Hyperglycemia exacerbates brain edema and perihematomal cell death after intracerebral hemorrhage. Stroke 34:2215–2220
Fein JM, Flor WJ, Cohan SL, Parkhurst J (1974) Sequential changes of vascular ultrastructure in experimental cerebral vasospasm. Myonecrosis of subarachnoid arteries. J Neurosurg 41:49–58
Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein HC (2001) Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke 32:2426–2432
Allport LE, Butcher KS, Baird TA, MacGregor L, Desmond PM, Tress BM, Colman P, Davis SM (2004) Insular cortical ischemia is independently associated with acute stress hyperglycemia. Stroke 35:1886–1891
Hamlin GP, Cernak I, Wixey JA, Vink R (2001) Increased expression of neuronal glucose transporter 3 but not glial glucose transporter 1 following severe diffuse traumatic brain injury in rats. J Neurotrauma 18:1011–1018
Oertel MF, Schwedler M, Stein M, Wachter D, Scharbrodt W, Schmidinger A, Boker DK (2007) Cerebral energy failure after subarachnoid hemorrhage: the role of relative hyperglycolysis. J Clin Neurosci 14:948–954
Bergsneider M, Hovda DA, Shalmon E, Kelly DF, Vespa PM, Martin NA, Phelps ME, McArthur DL, Caron MJ, Kraus JF, Becker DP (1997) Cerebral hyperglycolysis following severe traumatic brain injury in humans: a positron emission tomography study. J Neurosurg 86:241–251
Vespa P, Prins M, Ronne-Engstrom E, Caron M, Shalmon E, Hovda DA, Martin NA, Becker DP (1998) Increase in extracellular glutamate caused by reduced cerebral perfusion pressure and seizures after human traumatic brain injury: a microdialysis study. J Neurosurg 89:971–982
Vespa P, Boonyaputthikul R, McArthur DL, Miller C, Etchepare M, Bergsneider M, Glenn T, Martin N, Hovda D (2006) Intensive insulin therapy reduces microdialysis glucose values without altering glucose utilization or improving the lactate/pyruvate ratio after traumatic brain injury. Crit Care Med 34:850–856
Vespa PM, McArthur D, O'Phelan K, Glenn T, Etchepare M, Kelly D, Bergsneider M, Martin NA, Hovda DA (2003) Persistently low extracellular glucose correlates with poor outcome 6 months after human traumatic brain injury despite a lack of increased lactate: a microdialysis study. J Cereb Blood Flow Metab 23:865–877
Parkin M, Hopwood S, Jones DA, Hashemi P, Landolt H, Fabricius M, Lauritzen M, Boutelle MG, Strong AJ (2005) Dynamic changes in brain glucose and lactate in pericontusional areas of the human cerebral cortex, monitored with rapid sampling on-line microdialysis: relationship with depolarisation-like events. J Cereb Blood Flow Metab 25:402–413
Dreier JP, Woitzik J, Fabricius M, Bhatia R, Major S, Drenckhahn C, Lehmann TN, Sarrafzadeh A, Willumsen L, Hartings JA, Sakowitz OW, Seemann JH, Thieme A, Lauritzen M, Strong AJ (2006) Delayed ischaemic neurological deficits after subarachnoid haemorrhage are associated with clusters of spreading depolarizations. Brain 129:3224–3237
Dreier JP, Ebert N, Priller J, Megow D, Lindauer U, Klee R, Reuter U, Imai Y, Einhaupl KM, Victorov I, Dirnagl U (2000) Products of hemolysis in the subarachnoid space inducing spreading ischemia in the cortex and focal necrosis in rats: a model for delayed ischemic neurological deficits after subarachnoid hemorrhage? J Neurosurg 93:658–666
Acknowledgements
The authors are indebted to Sabine Seidlitz and Jasmin Kopetzki, our colleagues, and the nursing staff of the interdisciplinary intensive care unit for excellent support.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is discussed in the editorial available at: http://dx.doi.org/10.1007/s00134-008-1045-4.
Rights and permissions
About this article
Cite this article
Schlenk, F., Nagel, A., Graetz, D. et al. Hyperglycemia and cerebral glucose in aneurysmal subarachnoid hemorrhage. Intensive Care Med 34, 1200–1207 (2008). https://doi.org/10.1007/s00134-008-1044-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-008-1044-5