
Abstract
Purpose
The current study evaluates the demographic, clinical, and neurocognitive characteristics of a recruited FEP research sample, a research control group, and a FEP clinic sample that were assessed and treated within the same center and time period.
Methods
This study utilized data collected through an observational study and a retrospective chart review. Samples were ascertained in the Longitudinal Assessment and Monitoring of Clinical Status and Brain Function in Adolescents and Adults study and the Prevention and Recovery in Early Psychosis clinic. FEP clinic patients (n = 77), FEP research participants (n = 44), and age-matched controls (n = 38) were assessed using the MATRICS consensus cognitive battery and global functioning social and role scales. Between-group differences were assessed via one-way ANOVA and Chi-square analyses.
Results
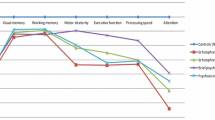
No significant differences were observed between groups with regard to age and gender. The FEP research sample had a higher proportion of white participants, better social and role functioning, and better neurocognitive performance when compared with the FEP clinical population. The clinic sample also had more diagnostic variability and higher prevalence of substance use disorders relative to the FEP research sample.
Conclusions
Researchers should be aware of how study design and recruitment practices may impact the representativeness of samples, with particular concern for equal representation of racial minorities and patients with more severe illness. Studies should be designed to minimize burden to promote a wider range of participation.


Similar content being viewed by others


References
Sue S (1999) Science, ethnicity, and bias: where have we gone wrong? Am Psychol 54:1070
Robinson D, Woerner MG, Pollack S et al (1996) Subject selection biases in clinical trials: data from a multicenter schizophrenia treatment study. J Clin Psychopharmacol 16:170–176
Longenecker J, Genderson J,et al (2010) Where have all the women gone? participant gender in epidemiological and non epidemiological research of schizophrenia. Schizophr Res 119:240–245
Chaves AC, Seeman MV (2006) Sex selection bias in schizophrenia antipsychotic trials. J Clin Psychopharmacol 26:489–494
Chakraborty BH, Steinhauer SR (2010) Reporting of minority participation rates and racial differences in schizophrenia and psychophysiological research: improving but still not adequate. Schizophr Res 123:90–91
Wendler D, Kington R, Madans J et al (2009) Are racial and ethnic minorities less willing to participate in health research? PLoS Med 3:e19
Hamilton LA, Aliyu MH, Lyons PD et al (2006) African-American community attitudes and perceptions toward schizophrenia and medical research: an exploratory study. J Natl Med Assoc 98:18
Thompson EE, Neighbors HW, Munday C et al (1996) Recruitment and retention of African American patients for clinical research: an exploration of response rates in an urban psychiatric hospital. J Consult Clin Psychol 64:861
Rothwell P (2005) External validity of randomized controlled trials: “to whom do the results of this trial apply?”. Lancet 365:82–93
Woodall A, Morgan C, Sloan C et al (2010) Barriers to participation in mental health research: are there specific gender, ethnicity and age related barriers? BMC Psychiatry 10:103
Friis S, Melle I, Larsen TK et al (2004) Does duration of untreated psychosis bias study samples of first-episode psychosis? Acta Psychiatr Scand 110:286–291
Marshall M, Lewis S, Lockwood A et al (2005) Association between duration of untreated psychosis and outcome in cohorts of first-episode patients: a systematic review. Arch Gen Psychiatry 62:975–983
Compton MT, Ramsay CE, Shim RS et al (2009) Health services determinants of the duration of untreated psychosis among African-American first-episode patients. Psychiatr Serv 60:1489–1494
Pope MA, Joober R, Malla AK (2013) Diagnostic stability of first-episode psychotic disorders and persistence of comorbid psychiatric disorders over 1 year. Can J Psychiatry 58:588–594
Khan AY, Preskorn SH, Baker B (2005) Effect of study criteria on recruitment and generalizability of the results. J Clin Psychopharmacol 25:271–275
Rabinowitz J, Bromet EJ, Davidson M (2003) Are patients enrolled in first episode psychosis drug trials representative of patients treated in routine clinical practice? Schizophr Res 61:149–155
Conus P, Cotton S, Schimmelmann BG et al (2017) Rates and predictors of 18-months remission in an epidemiological cohort of 661 patients with first-episode psychosis. Soc Psychiatry Psychiatr Epidemiol 1–1
Woodberry KA, Serur RA, Hallinan SB et al (2014) Frequency and pattern of childhood symptom onset reported by first episode schizophrenia and clinical high risk youth. Schizophr Res 158:45–51
Caplan B, Zimmet SV, Meyer EC et al (2013) Prevention and recovery in early psychosis (PREP1): building a public-academic partnership program in Massachusetts, united states. Asian J Psychiatr 6:171–177
Nuechterlein KH, Green MF, Kern RS et al (2008) The MATRICS Consensus Cognitive Battery, part 1: test selection, reliability, and validity. Am J Psychiatry 165:203–213
Cornblatt BA, Auther AM, Niendam T et al (2007) Preliminary findings for two new measures of social and role functioning in the prodromal phase of schizophrenia. Schizophr Bull 33:688–702
Kern RS, Nuechterlein KH, Green MF et al (2008) The MATRICS Consensus Cognitive Battery, part 2: co-norming and standardization. Am J Psychiatry 165:214–220
Wechsler D (2001) Wechsler test of adult reading: WTAR. Psychological Corporation, San Antonio
Wilkinson GS, Robertson GJ (2006) Wide range achievement test. Psychological Assessment Resources, Lutz, FL
Mullen CM, Fouty HE (2014) Comparison of the WRAT4 reading subtest and the WTAR for estimating premorbid ability level. Appl Neuropsychol Adult 21:69–72
Piskulic D, Addington J, Auther A et al (2011) Using the global functioning social and role scales in a first-episode sample. Early Interv Psychiatry 5:219–223
First MB, Spitzer RL, Gibbon M (2002) Structured clinical interview for DSM-IV-TR axis I disorders. Research version, patient edition. (SCID-I/P) New York. Psychiatric Institute, New York
Lobbestael J, Leurgans M, Arntz A (2011) Inter-rater reliability of the structured clinical interview for DSM-IV axis I disorders (SCID I) and axis II disorders (SCID II). Clin Psychol Psychother 18:75–79
Zanarini MC, Skodol AE, Bender D et al (2000) The collaborative longitudinal personality disorders study: reliability of axis I and II diagnoses. J Pers Disord 14:291–299, 2000
Hien D, Matzner FJ, First MB et al (1994) Structured clinical interview for DSM–IV–child edition (version 1.0). Columbia University, New York
Mesholam-Gately RI, Giuliano AJ, Goff KP et al (2009) Neurocognition in first-episode schizophrenia: a meta-analytic review. Neuropsychology 23:315–336
Marwaha S, Livingston G (2002) Stigma, racism or choice. why do depressed ethnic elders avoid psychiatrists? J Affect Disord 72:257–265
Varese F, Smeets F, Drukker M et al (2012) Childhood adversities increase the risk of psychosis: a meta-analysis of patient control, prospective-and cross-sectional cohort studies. Schizophr Bull 38:661–671
Longden E, Sampson M, Read J (2016) Childhood adversity and psychosis: generalised or specific effects? Epidemiol Psychiatr Sci 25:349–359
Schoenbaum M, Sutherland JM, Chappel A et al (2017) Twelve-month health care use and mortality in commercially insured young people with incident psychosis in the United States. Schizophr Bull 43:1262–1272
Acknowledgements
This work was supported in part by the National Institutes of Health via grants R01 MH103831, P50MH080272, UO1 MH081928, R01MH103831, R01MH102377, 1S10RR023401,1S10RR019307, and 1S10RR023043; by the Massachusetts Department of Mental Health (SCDMH82101008006); by a VA Merit Award (MES); by the National Alliance for Research in Schizophrenia and Depression via the Distinguished Investigator Award (MES), and by a Clinical Translational Science Award UL1RR025758 and General Clinical Research Center Grant M01RR01032 to Harvard University and Beth Israel Deaconess Medical Center from the National Center for Research Resources. We also wish to acknowledge the patients and their families for working with us in PREP® as well as the many individuals who contributed to the PREP® program, including Cynthia Berkowitz, Brina Caplan, Margaret Guyer, Jude Leung, Thomas Monteleone, and Ginger Smith. We also thank the clinical, research assistant, and data management staff from the Boston CIDAR study, including Caitlin Bryant, Ann Cousins, Grace Francis, Molly Franz, Lauren Gibson, Anthony Giuliano, Andréa Gnong-Granato, Maria Hiraldo, Sarah Hornbach, Kristy Klein, Grace Min, Corin Pilo-Comtois, Janine Rodenhiser-Hill, Julia Schutt, Shannon Sorensen, Reka Szent-Imry, Alison Thomas, Lynda Tucker, Chelsea Wakeham, and Kristen Woodberry.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical standards
All CIDAR participants provided informed consent prior to participating in the study. The use of de-identified data from the PREP® clinic for research has been approved by the Institutional Review Boards of Beth Israel Deaconess Medical Center and the Massachusetts Department of Mental Health.
Additional information
Drs. Robert W. McCarley and Larry J. Seidman are deceased.
Rights and permissions
About this article

Cite this article
Kline, E., Hendel, V., Friedman-Yakoobian, M. et al. A comparison of neurocognition and functioning in first episode psychosis populations: do research samples reflect the real world?. Soc Psychiatry Psychiatr Epidemiol 54, 291–301 (2019). https://doi.org/10.1007/s00127-018-1631-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-018-1631-x