
Abstract
Introduction
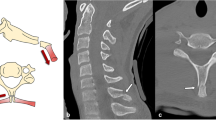
Traumatic neck pain is a common presentation to the emergency department. Lateral plain radiographs remain the primary investigation in the assessment of these injuries. Soft tissue assessment forms an integral component of these radiographs. They can provide information on subtle injuries that may not be obvious. Many methods are used to assess the prevertebral soft tissue shadows. The two more commonly used techniques include the ‘seven at two and two at seven’ rule (method 1) and the ratio of the soft tissues with respect to the vertebral width (method 2).
Aim
To assess which of the above two methods in assessing cervical spine soft tissue shadows on lateral radiographs is more sensitive in the presence of cervical spine injuries.
Methods
A retrospective analysis of consecutive traumatic cervical spine films performed within a busy trauma tertiary centre over a period of 7 months. Patients were divided into two groups: group 1—fractures; group 2—no fractures. The prevertebral soft tissue shadows were measured at referenced points on the lateral cervical spine films with respect to the above two methods and comparisons between the groups were made.
Results
Thirty-nine patients in group 1 were compared to a control group of 60 patients in group 2. Both methods failed to identify any significant differences between the two groups. The sensitivity and specificity for method 1 was 7.6 and 93 %, and for method 2, they were 7.6 and 98 %, respectively.
Conclusion
There is no significant difference between the soft tissue shadows when comparing patients with and without cervical spine fractures on lateral radiographs. Both commonly used measures of soft tissue shadows in clinical practice are insensitive in identifying patients with significant osseous injuries. They, therefore, do not offer any further value in interpreting traumatic cervical spine radiographs. The management of patients with cervical spine trauma in the absence of obvious osseous injury on standard radiographs should warrant a computed tomography (CT) scan if clinically indicated.





Similar content being viewed by others


References
Bailitz J, Starr F, Beecroft M, Bankoff J, Roberts R, Bokhari F, Joseph K, Wiley D, Dennis A, Gilkey S, Erickson P, Raksin P, Nagy K. CT should replace three-view radiographs as the initial screening test in patients at high, moderate, and low risk for blunt cervical spine injury: a prospective comparison. J Trauma. 2009;66(6):1605–9.
Di Mascio L, Sivaraman A. Cervical prevertebral soft tissue swelling in the traumatized patient: what is normality in the intubated patient? Eur J Trauma Emerg Surg. 2009;35(2):165–8.
Dai LY. Significance of prevertebral soft tissue measurement in cervical spine injuries. Eur J Radiol. 2004;51(1):73–6.
Penning L. Prevertebral hematoma in cervical spine injury: incidence and etiologic significance. AJR Am J Roentgenol. 1981;136:556–61.
McCormick CC. Prevertebral soft-tissue measurements in cervical spine injury: ‘seven at two; two at seven’. Australas Radiol. 1997;41:227–8.
Herdman RC, Saeed SR, Hinton EA. The lateral soft tissue neck X-ray in accident and emergency medicine. Arch Emerg Med. 1992;9:149–56.
Baren JM, Rothrock SG. Pediatric emergency medicine. Philadelphia: Elsevier; 2007.
Chen MY, Bohrer SP. Radiographic measurement of prevertebral soft tissue thickness on lateral radiographs of the neck. Skeletal Radiol. 1999;28(8):444–6.
Clark WM, Gehweiler JA Jr, Laib R. Twelve significant signs of cervical spine trauma. Skelet Radiol. 1979;3:201–5.
Hay PD. Annals of roentgenology, vol. 9. New York: Paul B Hoeber; 1939.
Dai LY. Significance of prevertebral soft tissue measurement in cervical spine injuries. Eur J Radiol. 2004;51(1):73–6.
DeBehnke DJ, Havel CJ. Utility of prevertebral soft tissue measurements in identifying patients with cervical spine fractures. Ann Emerg Med. 1994;24(6):1119–24.
Marar BC. Hyperextension injuries of the cervical spine. The pathogenesis of damage to the spinal cord. J Bone Joint Surg Am. 1974;56:1655–62.
Lusted LB, Keats TE. Atlas of roentgenographic measurement. 3rd ed. Chicago: Year Book; 1973.
Wholey MH, Bruwer AJ, Baker HL Jr. The lateral roentgenogram of the neck; with comments on the atlanto–odontoid–basion relationship. Radiology. 1958;71:350–6.
Markuske H. Radiologische Messungen der Retropharyngeal breite und des Retrotracheabraums im Kindesalter. Dtsch Gesundheitswes. 1978;33:1729–32.
Kendall BE, Ashcroft K, Whiteside CG. A physiological variation in the barium-filled gullet. Br J Radiol. 1962;35:769–75.
Matar LD, Doyle AJ. Prevertebral soft-tissue measurements in cervical spine injury. Australas Radiol. 1997;41:229–37.
Bandiera G, Stiell IG, Wells GA, Clement C, De Maio V, Vandemheen KL, Greenberg GH, Lesiuk H, Brison R, Cass D, Dreyer J, Eisenhauer MA, Macphail I, McKnight RD, Morrison L, Reardon M, Schull M, Worthington J; Canadian C-Spine and CT Head Study Group. The Canadian C-spine rule performs better than unstructured physician judgment. Ann Emerg Med. 2003;42(3):395–402.
Conflict of interest
There is no conflict of interest for this paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Patel, M.S., Grannum, S., Tariq, A. et al. Are soft tissue measurements on lateral cervical spine X-rays reliable in the assessment of traumatic injuries?. Eur J Trauma Emerg Surg 39, 613–618 (2013). https://doi.org/10.1007/s00068-013-0302-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-013-0302-6