
Abstract
Purpose
The nutritional status of inpatients influences the therapeutic outcome. Malnutrition is a common comorbidity in oncological patients. Both radio- and radiochemotherapy may contribute to the additional deterioration of the nutritional status. The aim of this study was to evaluate the impact of specialized treatment of malnutrition as a clinical routine.
Methods
The nutritional status of inpatients was assessed by the Nutritional risk screening (NRS-2002) on the day of admission to the University Department of Radiation Oncology. In case of significantly elevated NRS-2002 (NRS ≥ 3), a guideline-compliant, individual nutritional treatment was initiated by a specialized nutrition support team. The influence of the nutritional status and nutritional treatment on length of stay and complication rate was assessed.
Results
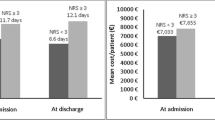
Of 840 included patients, 344 patients (40.95%) were at risk for malnutrition. Malnutrition was a significant, independent risk factor for both prolonged hospital stay, represented by the deviation between the actual length of stay and the DRG-associated mean length of stay (dLOS at risk: 0.88 days, dLOS not at risk: −0.88 days, p = 0.0047), as well as for the occurrence of complications (OR: 1.758 CI: [1.286–2.402], p = 0.0006). In the group of 337 (40.12%) rehospitalized patients the nutritional management was able to assimilate the values of length of stay as well as the complication rates to standard values.
Conclusions
The high risk for malnutrition and the negative consequences for patients and hospitals underline the urgent need for malnutrition screening on admission and treatment of malnutrition. A specialized, interdisciplinary nutrition support team positively influences patient outcome and should be established routinely in all oncological disciplines.
Zusammenfassung
Zweck
Der Ernährungszustand spielt für den Behandlungserfolg von stationären Patienten eine wichtige Rolle. Mangelernährung stellt bei onkologischen Patienten eine häufige Komorbidität dar. Sowohl Radiotherapien als auch Radiochemotherapien können zur zusätzlichen Verschlechterung des Ernährungszustands beitragen. Das primäre Ziel der Studie war es, den Einfluss eines in die klinische Routine eingebundenen standardisierten Ernährungsmanagements zu evaluieren.
Methoden
Bei stationären Patienten der Universitätsklinik für Radioonkologie wurde am Tag der Aufnahme der Ernährungszustand mittels des Nutritional Risk Score (NRS-2002) bewertet. Bei auffälligem Screening (NRS ≥ 3) wurde eine leitlinienkonforme individuelle Ernährungstherapie durch ein spezialisiertes Ernährungsteam eingeleitet. Der Einfluss des Ernährungszustands sowie der Ernährungstherapie auf Verweildauer und Komplikationsrate wurde bewertet.
Ergebnisse
Von 840 Patienten wiesen 344 (40,95%) ein erhöhtes Mangelernährungsrisiko auf. Mangelernährung wurde als signifikanter unabhängiger Risikofaktor sowohl für einen längeren Krankenhausaufenthalt, abgebildet durch die Differenz zwischen der tatsächlichen und der zur diagnosebezogenen Fallgruppe (DRG) gehörenden mittleren Verweildauer („DRG-associated mean length of stay“, dLOS mit Risiko: 0,88 Tage; dLOS ohne Risiko: −0,88 Tage; p = 0,0047), als auch für das Auftreten von Komplikationen nachgewiesen (Odds Ratio, OR: 1,758; 95%-Konfidenzintervall, 95%-KI: 1,286–2,402; p = 0,0006). Durch das Ernährungsmanagement wurden bei den 337 (40,12%) Patienten mit stationärer Wiederaufnahme im weiteren Verlauf sowohl die Verweildauer als auch die Komplikationsrate an Normwerte angeglichen.
Schlussfolgerung
Das hohe Mangelernährungsrisiko und die negativen Konsequenzen für Patienten und Klinik unterstreichen die Notwendigkeit eines Mangelernährungsscreenings bei Aufnahme sowie die anschließende Ernährungstherapie. Ein spezialisiertes, interdisziplinär arbeitendes Ernährungsteam beeinflusst das Patientenergebnis positiv und sollte in sämtlichen onkologischen Fachdisziplinen standardmäßig etabliert werden.




Similar content being viewed by others


References
Working Group on Prevention and Integrative Oncology (PRIO) (2016) Improving nutritional care for cancer patients in Germany. Joint position paper from the German Cancer Society‘s (GCS) Working Group on Prevention and Integrative Oncology (PRIO), in collaboration with other associations. Ernahr Umsch 63(02):43–47. https://doi.org/10.4455/eu.2016.011
Cepton Strategies (2007) Mangelernährung in Deutschland
Pirlich M, Schutz T, Norman K, Gastell S, Lubke HJ, Bischoff SC, Bolder U, Frieling T, Guldenzoph H, Hahn K, Jauch KW, Schindler K, Stein J, Volkert D, Weimann A, Werner H, Wolf C, Zurcher G, Bauer P, Lochs H (2006) The German hospital malnutrition study. Clin Nutr 25(4):563–572. https://doi.org/10.1016/j.clnu.2006.03.005
Thomas MN, Kufeldt J, Kisser U, Hornung HM, Hoffmann J, Andraschko M, Werner J, Rittler P (2016) Effects of malnutrition on complication rates, length of hospital stay, and revenue in elective surgical patients in the G‑DRG-system. Nutrition 32(2):249–254. https://doi.org/10.1016/j.nut.2015.08.021
Kisser U, Kufeldt J, Adderson-Kisser C, Becker S, Baumeister P, Reiter M, Harreus U, Thomas MN, Rittler P (2016) Clinical impact of malnutrition on complication rate and length of stay in elective ENT patients: a prospective cohort study. Eur Arch Otorhinolaryngol. https://doi.org/10.1007/s00405-016-3974-9
Rosenbaum A, Piper S, Riemann JF, Schilling D (2007) Mangelernährung bei internistischen Patienten – eine Screeninguntersuchung von 1308 Patienten mit Verlaufsbeobachtung. Aktuel Ernahrungsmed 32(04):181–184. https://doi.org/10.1055/s-2007-970921 (Malnutrition in Medical Patients – Screening of 1308 Patients and Follow-Up)
Bonetti L, Terzoni S, Lusignani M, Negri M, Froldi M, Destrebecq A (2017) Prevalence of malnutrition among older people in medical and surgical wards in hospital and quality of nutritional care: a multicenter, cross-sectional study. J Clin Nurs. https://doi.org/10.1111/jocn.14051
Planas M, Alvarez-Hernandez J, Leon-Sanz M, Celaya-Perez S, Araujo K, Garcia de Lorenzo A, PREDyCES® researchers (2016) Prevalence of hospital malnutrition in cancer patients: a sub-analysis of the PREDyCES(R) study. Support Care Cancer 24(1):429–435. https://doi.org/10.1007/s00520-015-2813-7
Unsal D, Mentes B, Akmansu M, Uner A, Oguz M, Pak Y (2006) Evaluation of nutritional status in cancer patients receiving radiotherapy: a prospective study. Am J Clin Oncol 29(2):183–188. https://doi.org/10.1097/01.coc.0000198745.94757.ee
Pressoir M, Desne S, Berchery D, Rossignol G, Poiree B, Meslier M, Traversier S, Vittot M, Simon M, Gekiere JP, Meuric J, Serot F, Falewee MN, Rodrigues I, Senesse P, Vasson MP, Chelle F, Maget B, Antoun S, Bachmann P (2010) Prevalence, risk factors and clinical implications of malnutrition in French Comprehensive Cancer Centres. Br J Cancer 102(6):966–971. https://doi.org/10.1038/sj.bjc.6605578
Sorensen J, Kondrup J, Prokopowicz J, Schiesser M, Krahenbuhl L, Meier R, Liberda M, EuroOOPS study group (2008) EuroOOPS: an international, multicentre study to implement nutritional risk screening and evaluate clinical outcome. Clin Nutr 27(3):340–349. https://doi.org/10.1016/j.clnu.2008.03.012
Harter J, Orlandi SP, Gonzalez MC (2017) Nutritional and functional factors as prognostic of surgical cancer patients. Support Care Cancer 25(8):2525–2530. https://doi.org/10.1007/s00520-017-3661-4
Burgos R, Sarto B, Elio I, Planas M, Forga M, Canton A, Trallero R, Munoz MJ, Perez D, Bonada A, Salo E, Lecha M, Enrich G, Salas-Salvado J, Group for the Study of Malnutrition in Hospitals in Catalonia (2012) Prevalence of malnutrition and its etiological factors in hospitals. Nutr Hosp 27(2):469–476. https://doi.org/10.1590/S0212-16112012000200018
Correia MI, Waitzberg DL (2003) The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin Nutr 22(3):235–239
Silver HJ, Dietrich MS, Murphy BA (2007) Changes in body mass, energy balance, physical function, and inflammatory state in patients with locally advanced head and neck cancer treated with concurrent chemoradiation after low-dose induction chemotherapy. Head Neck 29(10):893–900. https://doi.org/10.1002/hed.20607
Bozzetti F (2013) Nutritional support of the oncology patient. Crit Rev Oncol Hematol 87(2):172–200. https://doi.org/10.1016/j.critrevonc.2013.03.006
van den Berg MG, Rutten H, Rasmussen-Conrad EL, Knuijt S, Takes RP, van Herpen CM, Wanten GJ, Kaanders JH, Merkx MA (2014) Nutritional status, food intake, and dysphagia in long-term survivors with head and neck cancer treated with chemoradiotherapy: a cross-sectional study. Head Neck 36(1):60–65. https://doi.org/10.1002/hed.23265
Korner P, Ehrmann K, Hartmannsgruber J, Metz M, Steigerwald S, Flentje M, van Oorschot B (2017) Patient-reported symptoms during radiotherapy: clinically relevant symptom burden in patients treated with palliative and curative intent. Strahlenther Onkol 193(7):570–577. https://doi.org/10.1007/s00066-017-1146-5
Alterio D, Gerardi MA, Cella L, Spoto R, Zurlo V, Sabbatini A, Fodor C, D’Avino V, Conson M, Valoriani F, Ciardo D, Pacelli R, Ferrari A, Maisonneuve P, Preda L, Bruschini R, Cossu Rocca M, Rondi E, Colangione S, Palma G, Dicuonzo S, Orecchia R, Sanguineti G, Jereczek-Fossa BA (2017) Radiation-induced acute dysphagia: prospective observational study on 42 head and neck cancer patients. Strahlenther Onkol 193(11):971–981. https://doi.org/10.1007/s00066-017-1206-x
Martin L, Senesse P, Gioulbasanis I, Antoun S, Bozzetti F, Deans C, Strasser F, Thoresen L, Jagoe RT, Chasen M, Lundholm K, Bosaeus I, Fearon KH, Baracos VE (2015) Diagnostic criteria for the classification of cancer-associated weight loss. J Clin Oncol 33(1):90–99. https://doi.org/10.1200/JCO.2014.56.1894
Kondrup J, Rasmussen HH, Hamberg O, Stanga Z, Ad Hoc ESPEN Working Group (2003) Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutr 22(3):321–336
Arends J, Bertz H, Bischoff SC, Fietkau R, Herrmann HJ, Holm E, Horneber M, Hütterer E, Körber J, Schmid I, und das DSC (2015) S3-Leitline der Deutschen Gesellschaft für Ernährungsmedizin e. V. (DGEM) in Kooperation mit der Deutschen Gesellschaft für Hämatologie und Onkologie e. V. (DGHO), der Arbeitsgemeinschaft „Supportive Maßnahmen in der Onkologie, Rehabilitation und Sozialmedizin“ der Deutschen Krebsgesellschaft (ASORS) und der Österreichischen Arbeitsgemeinschaft für klinische Ernährung (AKE) (S3-Guideline of the German Society for Nutritional Medicine (DGEM) in Cooperation with the DGHO, the ASORS and the AKE). Aktuel Ernahrungsmed 40 (05):e1–e74. https://doi.org/10.1055/s-0035-1552741
Kufeldt J, Kovarova M, Adolph M, Staiger H, Bamberg M, Haring HU, Fritsche A, Peter A (2017) Prevalence and distribution of diabetes mellitus in a maximum care hospital: urgent need for HbA1c-screening. Exp Clin Endocrinol Diabetes. https://doi.org/10.1055/s-0043-112653
Deutsches Institut für Medizinische Dokumentation und Information (DIMDI) im Auftrag des Bundesministeriums für Gesundheit (BMG) unter Beteiligung der Arbeitsgruppe ICD des Kuratoriums für Fragen der Klassifikation im Gesundheitswesen (2018) ICD-10-GM Version 2018. Systematisches Verzeichnis Internationale statistische Klassifikation der Krankheiten und verwandter Gesundheitsprobleme (10. Revision, German modification). https://www.dimdi.de/static/de/klassifikationen/icd/icd-10-gm/kode-suche/htmlgm2018/
Kuppinger D, Hartl WH, Bertok M, Hoffmann JM, Cederbaum J, Bender A, Küchenhoff H, Rittler P (2013) Nutritional screening for risk prediction in patients scheduled for extra-abdominal surgery. Nutrition 29(2):399–404. https://doi.org/10.1016/j.nut.2012.06.013
Fietkau R (2016) Einfluss der Ernährung bei Strahlen- und Radiochemotherapie. Onkologe 22(4):268–274. https://doi.org/10.1007/s00761-016-0012-x
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J. Kufeldt reports a doctoral scholarship from B. Braun Melsungen AG, during the conduct of the study and outside the submitted work. No other potential conflicts of interest relevant to this article were reported. B. Braun had no involvement in the study design, data collection and analysis or writing of the manuscript. M. Viehrig, D. Schweikert, A. Fritsche, M. Bamberg and M. Adolph declare that they have no competing interests.
Caption Electronic Supplementary Material
Rights and permissions
About this article

Cite this article
Kufeldt, J., Viehrig, M., Schweikert, D. et al. Treatment of malnutrition decreases complication rates and shortens the length of hospital stays in a radiation oncology department. Strahlenther Onkol 194, 1049–1059 (2018). https://doi.org/10.1007/s00066-018-1360-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-018-1360-9