
Purpose:
To evaluate the accuracy of virtual simulation, which is less time-consuming than physical simulation, with the new laser system Dorado CT4 in 96 prostate cancer patients.
Patients and Methods:
Virtual simulation was based on a spiral scan with 8 mm reconstruction index and 8 mm slice thickness in 64 patients (group A), and 3 mm reconstruction index and 3 mm slice thickness in 32 patients (group B). Both groups were evaluated for impact on maximum difference (Δmax) regarding the isocenters obtained from virtual simulation versus those obtained from physical simulation.
Results:
In the entire cohort, mean differences were as follows: Δmax 5.7 ± 3.5 mm, Δx (left/right) 2.8 ± 2.9 mm, Δy (anterior/posterior) 4.5 ± 3.8 mm, and Δz (cranial/caudal) 2.1 ± 2.2 mm. In group A, mean values were Δmax 6.2 ± 3.8 mm, Δx 2.9 ± 3.1 mm, Δy 4.9 ± 4.2 mm, and Δz 2.3 ± 2.3 mm. In group B, mean values were Δmax 4.8 ± 2.8 mm, Δx 2.7 ± 2.7 mm, Δy 3.7 ± 2.7 mm, and Δz 1.7 ± 2.0 mm. Time of radiotherapy (primary vs. salvage RT) and radiation regimen (external-beam radiotherapy [EBRT] vs. high-dose-rate brachytherapy [HDR-BT] plus EBRT) had no significant impact on Δmax.
Conclusion:
Virtual simulation with the new laser system Dorado CT4 was very precise for both primary and salvage RT in the treatment of prostate cancer patients. High precision was achieved for both EBRT and HDR-BT plus EBRT. Virtual simulation should be performed with a planning CT with 3 mm reconstruction index and 3 mm slice thickness for high accuracy.
Hintergrund und Ziel:
Diese Studie untersucht die Präzision der virtuellen Simulation mit dem neuen Lasersystem Dorado CT4 bei 96 Patienten mit Prostatakarzinom.
Patienten und Methodik:
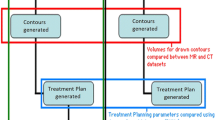
Die virtuelle Simulation (Abbildung 1) basierte bei 64 Patienten (Gruppe A) auf einem Spiral-CT mit 8 mm Schichtdicke und 8 mm Rekonstruktionsindex, bei 32 Patienten (Gruppe B) auf einem Spiral-CT mit 3 mm Schichtdicke und 3 mm Rekonstruktionsindex (Tabelle 1). Beide Gruppen wurden hinsichtlich der maximalen Differenz (Δmax) zwischen den Isozentren der virtuellen Simulation und den Isozentren der konventionellen Simulation verglichen.
Ergebnisse:
Im Gesamtkollektiv waren die mittleren Differenzen folgendermaßen: Δmax 5,7 ± 3,5 mm, Δx (links/rechts) 2,8 ± 2,9 mm, Δy (anterior/posterior) 4,5 ± 3,8 mm, Δz (kranial/kaudal) 2,1 ± 2,2 mm (Tabelle 2). In Gruppe A ergaben sich folgende Mittelwerte: Δmax 6,2 ± 3,8 mm, Δx 2,9 ± 3,1 mm, Δy 4,9 ± 4,2 mm, Δz 2,3 ± 2,3 mm. Die Mittelwerte in Gruppe B waren 4,8 ± 2,8 mm für Δmax, 2,7 ± 2,7 mm für Δx, 3,7 ± 2,7 mm für Δy und 1,7 ± 2,0 mm für Δz. Der Zeitpunkt der Strahlentherapie (primäre vs. Salvage-RT) und das RT-Regime (perkutane RT vs. High-Dose-Rate-Brachytherapie [HDR-BT] plus perkutane RT) hatten keinen signifikanten Einfluss auf Δmax (Tabelle 3).
Schlussfolgerung:
Die virtuelle Simulation mit dem Lasersystem Dorado CT4 bei der RT von Patienten mit Prostatakarzinom ist sehr präzise, und zwar unabhängig vom Zeitpunkt der RT (primäre RT, Salvage-RT) und vom RT-Regime (perkutane RT, HDR-BT plus perkutane RT). Schichtdicke und Rekonstruktionsindex des für die virtuelle Simulation verwendeten Planungs-CT sollten 3 mm betragen, um eine hohe Präzision zu erreichen.
Similar content being viewed by others


Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rades, D., Frenzel, T., Schwarz, R. et al. High Accuracy of Virtual Simulation with the Laser System Dorado CT4. Strahlenther Onkol 183, 89–93 (2007). https://doi.org/10.1007/s00066-007-1610-8
Received:
Revised:
Issue Date:
DOI: https://doi.org/10.1007/s00066-007-1610-8