
Background:
The use of the belly board device (BBD) in the prone position has gained acceptance to spare small bowel in rectal cancer patients irradiated postoperatively, but there are few data in the preoperative setting, and the advantages of the BBD regarding normal tissue sparing may be counteracted by problems of patient positioning. This study was undertaken to investigate prospectively the influence of the BBD on treatment reproducibility in patients irradiated preoperatively in the prone position.
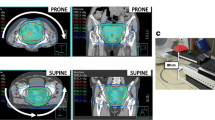
Patients and Methods: 23 patients with rectal carcinoma in clinical stages II/III were included in this study. Axis displacement was evaluated in 14 patients treated without the BBD and nine with. The BBD is a commercial device (Belly Board, Radiation Products Design, Albertville, MN) made of a 17-cm thick hard sponge with an opening of 42 × 42 cm2. No specific patient immobilization devices were used. During radiotherapy, twelve patients had four control films, while eleven patients had three. The mean treatment position deviation was calculated for the medio-lateral, cranio-caudal and antero-posterior directions.
Results: When comparing the first control film to the corresponding simulation film for patients without the BBD and with the BBD, the mean lateral displacements were 1.5 mm and 3.2 mm (p = 0.26), the mean cranio-caudal displacments were 1.55 mm and 4.2 mm (p = 0.13), and the mean antero-posterior displacements were 1.8 mm and 4.5 mm (p = 0.04), respectively. When considering all control films, for the three directions, the amplitudes of the displacements were greater when using the BBD, particularly for the antero-posterior direction where the difference was highly significant (p = 0.0006).
Conclusions: Our data show that, in patients treated prone for rectal cancer, the use of the BBD in the preoperative setting without immobilization devices was associated with problems of patient position reproducibility, particularly for the antero-posterior direction. Thus, the use of patient immobilization devices and/or individual custom-made BBD may be recommended if a decision to treat the patient with a BBD is taken.
Hintergrund:
In der postoperativen Radiotherapie des Rektumkarzinoms gilt die Anwendung des Bauchbretts in Bauchlage als etablierte Hilfe, um den Dünndarm auszusparen. Es gibt jedoch wenig Daten über die präoperative Anwendung des Bauchbretts. Der Vorteil des Bauchbrett, gesundes Gewebe auszusparen, könnte durch den Nachteil der erschwerten Reproduzierbarkeit der Patientenlagerung aufgewogen werden. Diese prospektive Studie hatte zum Ziel, bei präoperativ in Bauchlage bestrahlten Patienten den Einfluss des Bauchbretts auf die Reproduzierbarkeit der Patientenlagerung zu untersuchen.
Patienten und Methode: 23 Patienten mit einem Rektumkarzinom im klinischen Stadium II/II wurden in diese Studie eingeschlossen. Die Achsenabweichung wurde bei 14 Patienten ohne Bauchbrett und in neun Patienten mit Bauchbrett untersucht. Das Bauchbrett ist kommerziell erhältlich (Belly Board, Radiation Products Design, Albertville, MN). Es besteht aus einem harten Schwamm mit einer Dicke von 17 cm und einer Öffnung von 42 × 42 cm2. Keine weiteren spezifischen Hilfsmittel zur Immobilisation wurden verwendet. Während der Radiotherapie wurden bei zwölf Patienten je vier und bei elf Patienten je drei Kontrollbilder angefertigt. Die durchschnittliche Abweichung der Behandlungsposition wurde für die mediolaterale und die anteroposteriore Achse berechnet.
Ergebnisse: Wurde das erste Kontrollbild mit dem Simulatorbild verglichen, so lag die durchschnittliche Abweichung in der lateralen Abweichung bei 1,5 mm für Patienten, welche ohne Bauchbrett behandelt wurden, gegenüber 3,2 mm für Patienten, welche mit Bauchbrett behandelt wurden (p = 0,26). Die durchschnittliche kraniokaudale Abweichung lag bei 1,55 (ohne Bauchbrett) und 4,2 mm (mit Bauchbrett) (p = 0,13). Die durchschnittliche Abweichung in der anteroposterioren Achse lag bei 1,8 mm (ohne Bauchbrett) und 4,5 mm (mit Bauchbrett) (p = 0,04). Wenn alle Kontrollbilder in allen drei Achsen betrachtet wurden, so war die Abweichung bei Patienten, welche mit Bauchbrett behandelt wurden, am ausgeprägtesten. Die Differenz war am größten in der anteroposterioren Achse und auch statistisch hoch signifikant (p = 0,0006).
Schlussfolgerungen: Unsere Studie zeigt, dass bei Patienten, die wegen eines Rektumkarzinoms präoperativ in Bauchlage bestrahlt werden, die Anwendung des Bauchbretts ohne weitere Immobilisation zu Abweichungen in der Reproduzierbarkeit der Patientenpositionierung, speziell in der anteroposterioren Achse, führt. Darum empfehlen wir, falls man sich zum Gebrauch eines Bauchbretts entschließt, die Anwendung von Immobilisationshilfen und/oder einem individuell angefertigten Bauchbrett.
Similar content being viewed by others


Author information
Authors and Affiliations
Additional information
Received: May 15, 2001; accepted: February 20, 2002
Rights and permissions
About this article
Cite this article
Allal, A., Bischof, S. & Nouet, P. Impact of the “Belly Board” Device on Treatment Reproducibility in Preoperative Radiotherapy for Rectal Cancer. Strahlenther Onkol 178, 259–262 (2002). https://doi.org/10.1007/s00066-002-0889-8
Issue Date:
DOI: https://doi.org/10.1007/s00066-002-0889-8